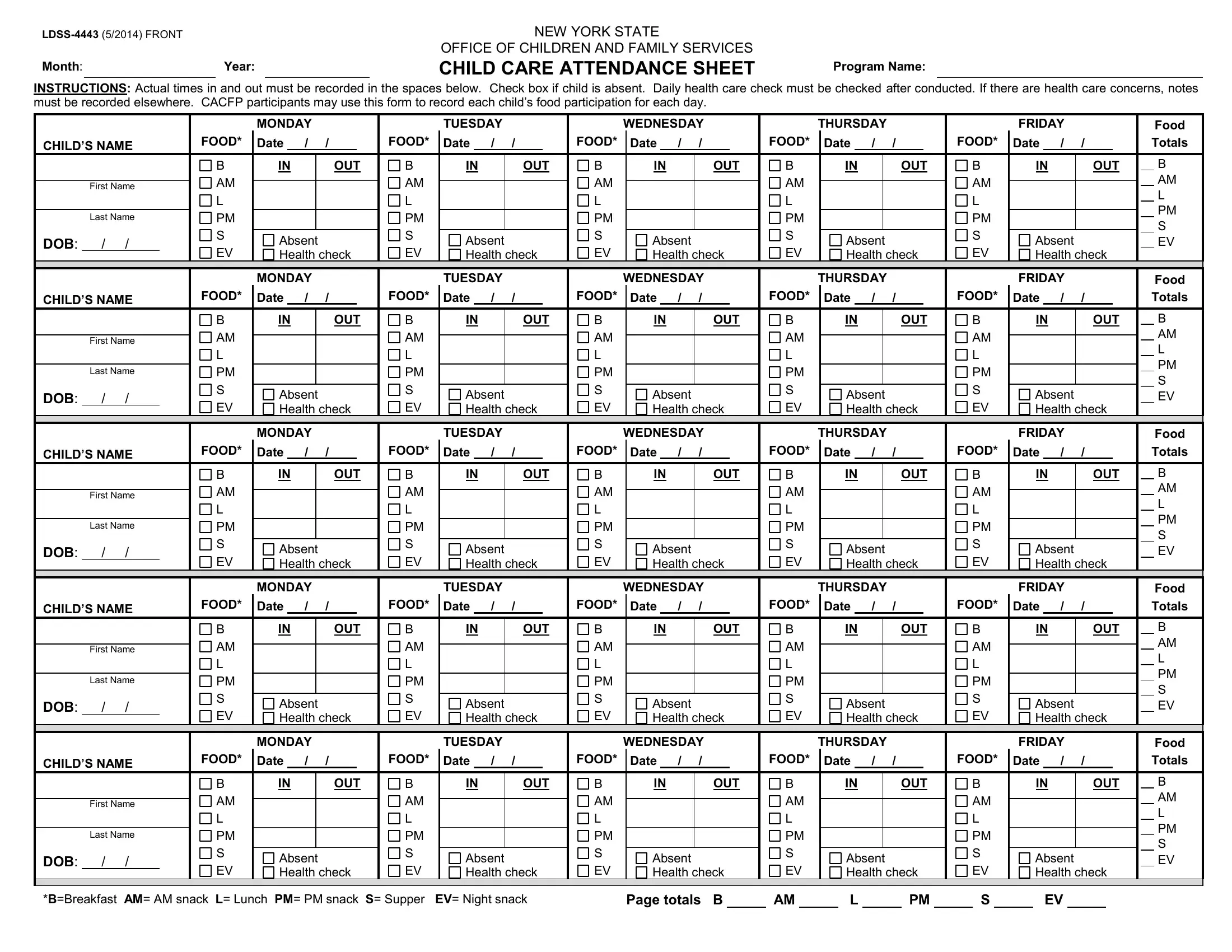
In the bustling world of child care facilities, meticulous records play a critical role in ensuring the health, safety, and well-being of children. The LDSS-4443 form, originating from the New York State Office of Children and Family Services, epitomizes this meticulous approach towards child care management. Designed to be utilized monthly, this form meticulously records each child's daily attendance, meal and snack participation, and crucially, the execution of daily health checks. Each section of the form allows for detailed entry of in and out times, marking absences, and specifying the types of meals provided—ranging from breakfast (B), AM and PM snacks, lunch (L), supper (S), to even evening snacks (EV). This structured documentation not only facilitates the smooth operation of child care programs but also ensures compliance with health standards and nutrition guidelines, particularly for participants of the Child and Adult Care Food Program (CACFP). In essence, the LDSS-4443 form serves as a comprehensive tool for child care providers to manage and monitor the essential aspects of child care that contribute to a nurturing and safe environment.
| Question | Answer |
|---|---|
| Form Name | Ldss 4443 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ocfs child care attendance sheet, ldss 4443 pdf, ldss 4443, ocfs attendance sheet |
NEW YORK STATE
OFFICE OF CHILDREN AND FAMILY SERVICES
Month: |
|
Year: |
|
CHILD CARE ATTENDANCE SHEET |
Program Name: |
INSTRUCTIONS: Actual times in and out must be recorded in the spaces below. Check box if child is absent. Daily health care check must be checked after conducted. If there are health care concerns, notes must be recorded elsewhere. CACFP participants may use this form to record each child’s food participation for each day.
|
|
|
|
|
|
|
|
|
MONDAY |
|
|
|
|
|
|
TUESDAY |
|
|
|
|
|
WEDNESDAY |
|
|
|
|
THURSDAY |
|
|
|
|
|
|
|
|
FRIDAY |
|
|
|
|
|
Food |
|||||||||||||||||||
|
|
CHILD’S NAME |
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
Totals |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
B |
IN |
|
|
OUT |
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
|
OUT |
|
B |
|
IN |
|
|
OUT |
|
|
B |
||||||||||||||||||
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|||
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|||||||||||
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
||||||||
|
|
|
Last Name |
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|||||||||||
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
||||||||||||||||||||||
|
|
DOB: |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EV |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
EV |
Health check |
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
EV |
|
Health check |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
MONDAY |
|
|
|
|
|
|
TUESDAY |
|
|
|
|
|
WEDNESDAY |
|
|
|
|
THURSDAY |
|
|
|
|
|
|
|
|
FRIDAY |
|
|
|
|
|
Food |
|||||||||||||||||||
|
|
CHILD’S NAME |
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
Totals |
|||||||||
|
|
|
|
|
|
|
|
B |
IN |
|
|
OUT |
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
|
OUT |
|
B |
|
IN |
|
|
OUT |
|
|
B |
||||||||||||||||||
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|||
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|||||||||||
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
||||||||
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|||||||||||
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
||||||||||||||||||||||
|
|
DOB: |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EV |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
EV |
Health check |
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
EV |
|
Health check |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
MONDAY |
|
|
|
|
|
|
TUESDAY |
|
|
|
|
|
WEDNESDAY |
|
|
|
|
THURSDAY |
|
|
|
|
|
|
|
|
FRIDAY |
|
|
|
|
|
Food |
|||||||||||||||||||
|
|
CHILD’S NAME |
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
Totals |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
B |
IN |
|
|
OUT |
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
|
OUT |
|
B |
|
IN |
|
|
OUT |
|
|
B |
||||||||||||||||||
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|||
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|||||||||||
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
||||||||
|
|
|
Last Name |
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|||||||||||
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
||||||||||||||||||||||
|
|
DOB: |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EV |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
EV |
Health check |
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
EV |
|
Health check |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
MONDAY |
|
|
|
|
|
|
TUESDAY |
|
|
|
|
|
WEDNESDAY |
|
|
|
|
THURSDAY |
|
|
|
|
|
|
|
|
FRIDAY |
|
|
|
|
|
Food |
|||||||||||||||||||
|
|
CHILD’S NAME |
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
Totals |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
B |
IN |
|
|
OUT |
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
|
OUT |
|
B |
|
IN |
|
|
OUT |
|
|
B |
||||||||||||||||||
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|||
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|||||||||||
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
||||||||
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|||||||||||
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
||||||||||||||||||||||
|
|
DOB: |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EV |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
EV |
Health check |
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
EV |
|
Health check |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MONDAY |
|
|
|
|
|
|
TUESDAY |
|
|
|
|
|
WEDNESDAY |
|
|
|
|
THURSDAY |
|
|
|
|
|
|
|
|
FRIDAY |
|
|
|
|
|
Food |
|||||||||||||||||||
|
|
CHILD’S NAME |
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
FOOD* |
|
Date |
|
/ |
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
|
FOOD* |
Date |
|
/ |
|
/ |
|
|
|
Totals |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
B |
IN |
|
|
OUT |
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
OUT |
|
|
B |
|
IN |
|
|
OUT |
|
B |
|
IN |
|
|
OUT |
|
|
B |
||||||||||||||||||
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
AM |
|||
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
L |
|||||||||||
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
L |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
||||||||
|
|
|
Last Name |
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|||||||||||
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
|
Absent |
|
|
|
|
|
||||||||||||||||||||||
|
|
DOB: |
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EV |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
EV |
Health check |
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
|
EV |
|
Health check |
|
EV |
|
Health check |
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
*B=Breakfast AM= AM snack L= Lunch PM= PM snack S= Supper |
EV= Night snack |
|
|
|
|
Page totals B |
|
|
|
AM |
|
|
L |
|
|
|
PM |
|
|
|
S |
|
|
|
EV |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||