We've used the hard work of our best developers to build the PDF editor you are about to work with. The software allows you to fill out the soonerride mileage reimbursement form document without any difficulty and don’t waste time. All you need to undertake is keep up with the following quick tips.
Step 1: The first step will be to hit the orange "Get Form Now" button.
Step 2: Now you are on the document editing page. You can edit, add information, highlight specific words or phrases, put crosses or checks, and add images.
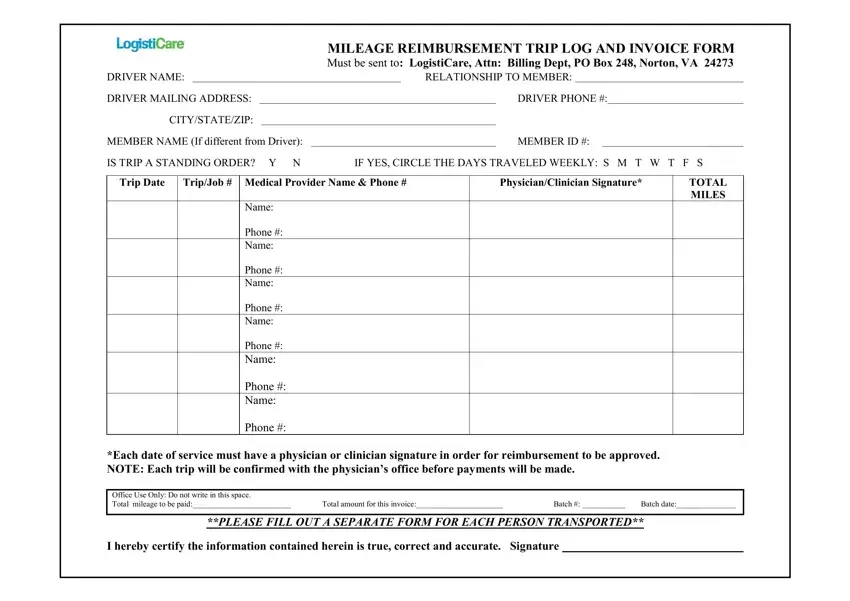
Type in the appropriate information in every single area to get the PDF soonerride mileage reimbursement form
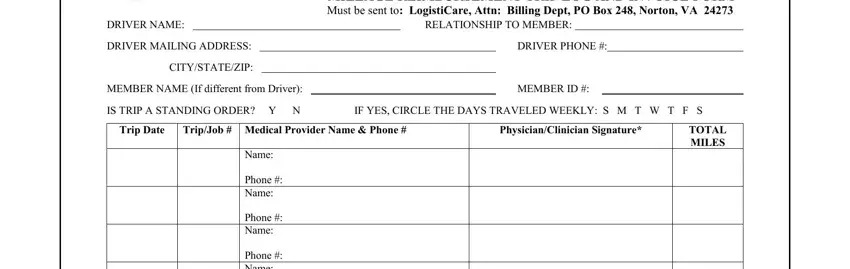
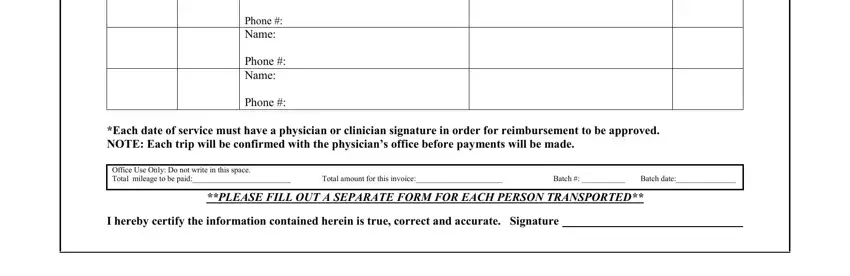
Type in the details in the Phone Name, Phone Name, Phone Name, Phone, Each date of service must have a, Office Use Only Do not write in, Total amount for this invoice, Batch, Batch date, PLEASE FILL OUT A SEPARATE FORM, and I hereby certify the information area.
Step 3: Once you click on the Done button, the finished file is readily exportable to each of your gadgets. Alternatively, you can easily deliver it using email.
Step 4: You can create duplicates of the file tostay clear of any type of possible future difficulties. Don't be concerned, we do not display or check your data.
