
It shouldn’t be challenging to prepare united healthcare oxford gym reimbursement through our PDF editor. This is how you can simply develop your form.
Step 1: Select the "Get Form Now" button to begin.
Step 2: When you have entered the editing page united healthcare oxford gym reimbursement, you'll be able to discover every one of the functions readily available for the file inside the upper menu.
The next few sections are what you will need to fill out to obtain the finished PDF document.
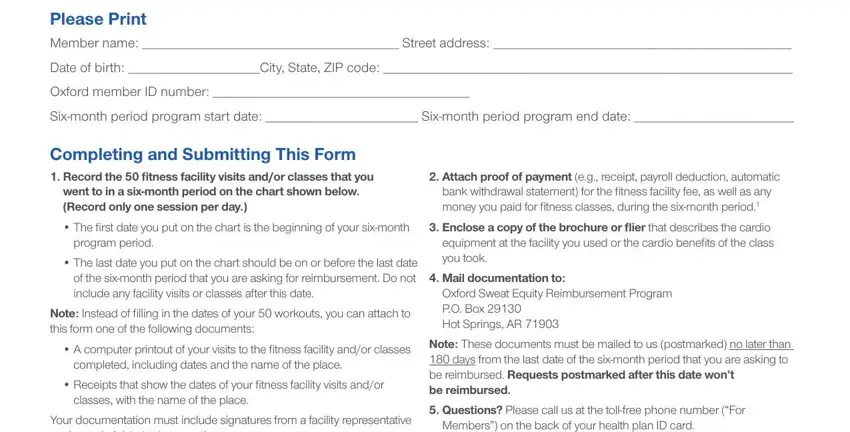
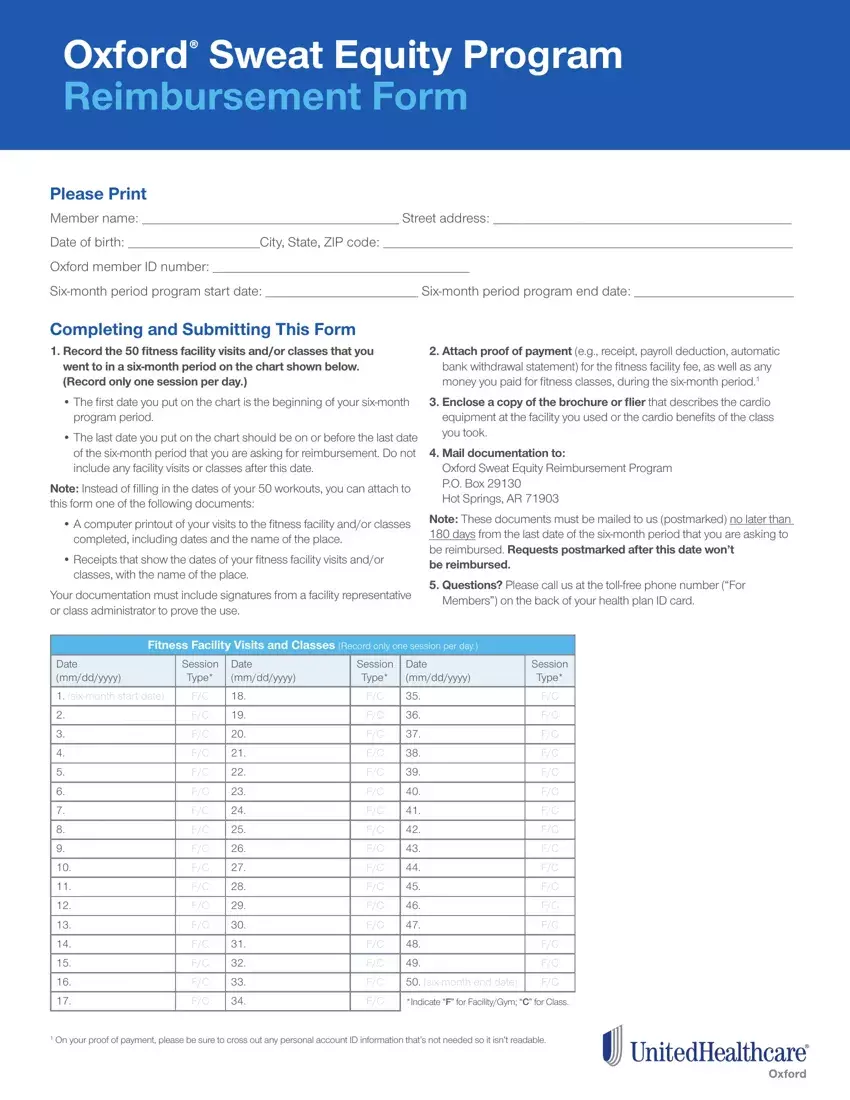
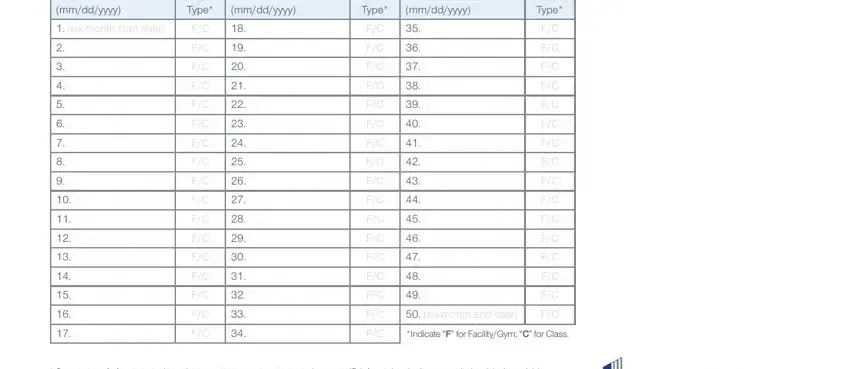
The software will need you to submit the Date mmddyyyy, Session Type, Date mmddyyyy, Session Type, Date mmddyyyy, Session Type, sixmonth start date, sixmonth end date, Indicate F for FacilityGym C for, and On your proof of payment please area.
You will have to include particular particulars in the space Fitness Facility Information, Facility name, Facility name if a second facility, Facility type, Facility type, Address Address, City State ZIP code City State, Telephone number, Telephone number, Fitness ClassSession Information, Fitness CenterInstructor, Signature Date, and Instructor or other facility.
It is essential to indicate the rights and responsibilities of both sides in part My signature below confirms that, Signature of Sweat Equity member, Exclusions and Limitations, of the member and his or her, For this program the use of you, refers to the Oxford plan, Refer to your Certificate of, governing member document to, To be eligible for reimbursement, facility or classes that you, You must be an active employee at, reimbursement We will reimburse, You must hold an active fitness, Memberships in tennis clubs, and Lifetime memberships are not.
Step 3: Press the "Done" button. Now it's possible to upload your PDF form to your electronic device. Aside from that, you can easily forward it via email.
Step 4: You could make duplicates of the document torefrain from any upcoming challenges. You should not worry, we don't distribute or check your information.
