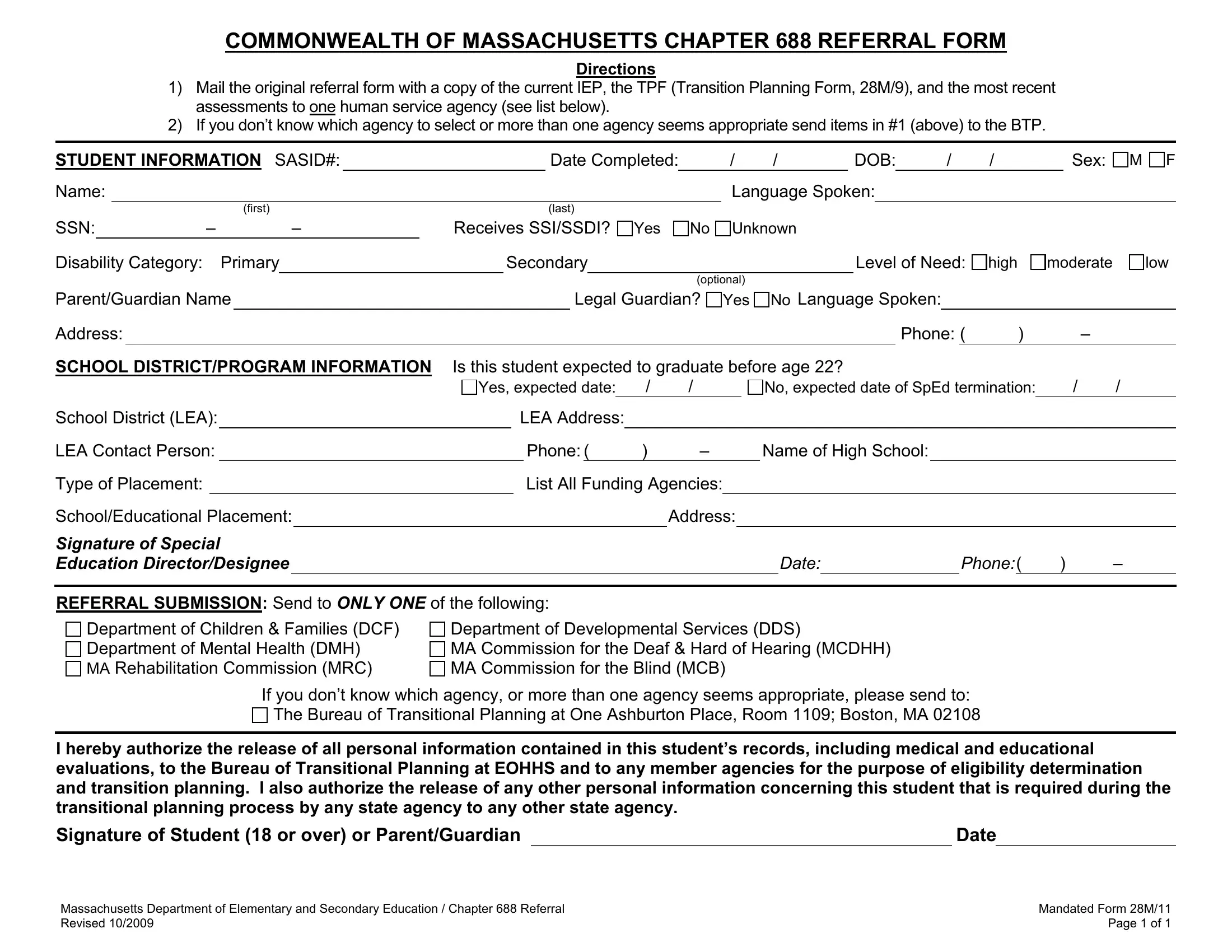
Navigating through the transition from school to the world of adulthood entails meticulous planning, especially for students with disabilities. In Massachusetts, the Mandated 28M/11 form, an essential document under Chapter 688, also known as the "Turning 22" law, plays a pivotal role in this transition. This form is designed to streamline the referral process to appropriate human service agencies, ensuring that the necessary support structures are in place as these students step into adulthood. The referral form, to be filled out alongside the current Individual Education Plan (IEP) and the Transition Planning Form (28M/9), requires detailed student information, including educational background and disability category, aiming to facilitate a seamless shift to post-secondary services. By mandating the submission of this form, along with the most recent assessments, to a single human service agency—or the Bureau of Transitional Planning if the best fit is unclear—the Commonwealth of Massachusetts underscores the importance of a coordinated approach in meeting the diverse needs of transitioning students. Moreover, the inclusion of explicit consent for the release of personal records emphasizes confidentiality and the student's autonomy in the process, ensuring a student-centered pathway to the future.
| Question | Answer |
|---|---|
| Form Name | Mandated Form 28M 11 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | MCDHH, 2009, SSN, SSDI |
COMMONWEALTH OF MASSACHUSETTS CHAPTER 688 REFERRAL FORM
Directions
1)Mail the original referral form with a copy of the current IEP, the TPF (Transition Planning Form, 28M/9), and the most recent assessments to one human service agency (see list below).
2)If you don’t know which agency to select or more than one agency seems appropriate send items in #1 (above) to the BTP.
STUDENT INFORMATION SASID#: |
|
Date Completed: |
/ |
/ |
DOB: |
/ |
/ |
Sex: |
|||
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
Language Spoken: |
|
|
|
||||
|
(first) |
|
(last) |
|
|
|
|
|
|
|
|
M F
SSN: |
|
– |
|
– |
Receives SSI/SSDI? Yes |
No Unknown |
|||
Disability Category: |
|
Primary |
|
Secondary |
|
Level of Need: |
|||
|
|
|
|
|
|
|
|
(optional) |
|
high
moderate
low
Parent/Guardian Name |
|
Legal Guardian? |
Address:
Yes No Language Spoken:
Phone: ( ) –
SCHOOL DISTRICT/PROGRAM INFORMATION |
Is this student expected to graduate before age 22? |
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
Yes, expected date: |
|
/ |
/ |
|
|
|
No, expected date of SpEd termination: |
/ |
/ |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
School District (LEA): |
|
|
LEA Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
LEA Contact Person: |
|
|
|
Phone:( |
|
) |
– |
|
Name of High School: |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Type of Placement: |
|
|
|
|
List All Funding Agencies: |
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
School/Educational Placement: |
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
||||
Signature of Special |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Education Director/Designee |
|
|
|
|
|
|
|
|
|
|
|
|
DATE: |
|
PHONE:( |
) |
– |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REFERRAL SUBMISSION: Send to ONLY ONE of the following:
Department of Children & Families (DCF)
Department of Mental Health (DMH)
MA Rehabilitation Commission (MRC)
Department of Developmental Services (DDS)
MA Commission for the Deaf & Hard of Hearing (MCDHH) MA Commission for the Blind (MCB)
If you don’t know which agency, or more than one agency seems appropriate, please send to:
The Bureau of Transitional Planning at One Ashburton Place, Room 1109; Boston, MA 02108
I hereby authorize the release of all personal information contained in this student’s records, including medical and educational evaluations, to the Bureau of Transitional Planning at EOHHS and to any member agencies for the purpose of eligibility determination and transition planning. I also authorize the release of any other personal information concerning this student that is required during the transitional planning process by any state agency to any other state agency.
Signature of Student (18 or over) or Parent/Guardian |
|
Date |
|
|
|
|
|
Massachusetts Department of Elementary and Secondary Education / Chapter 688 Referral |
Mandated Form 28M/11 |
Revised 10/2009 |
Page 1 of 1 |