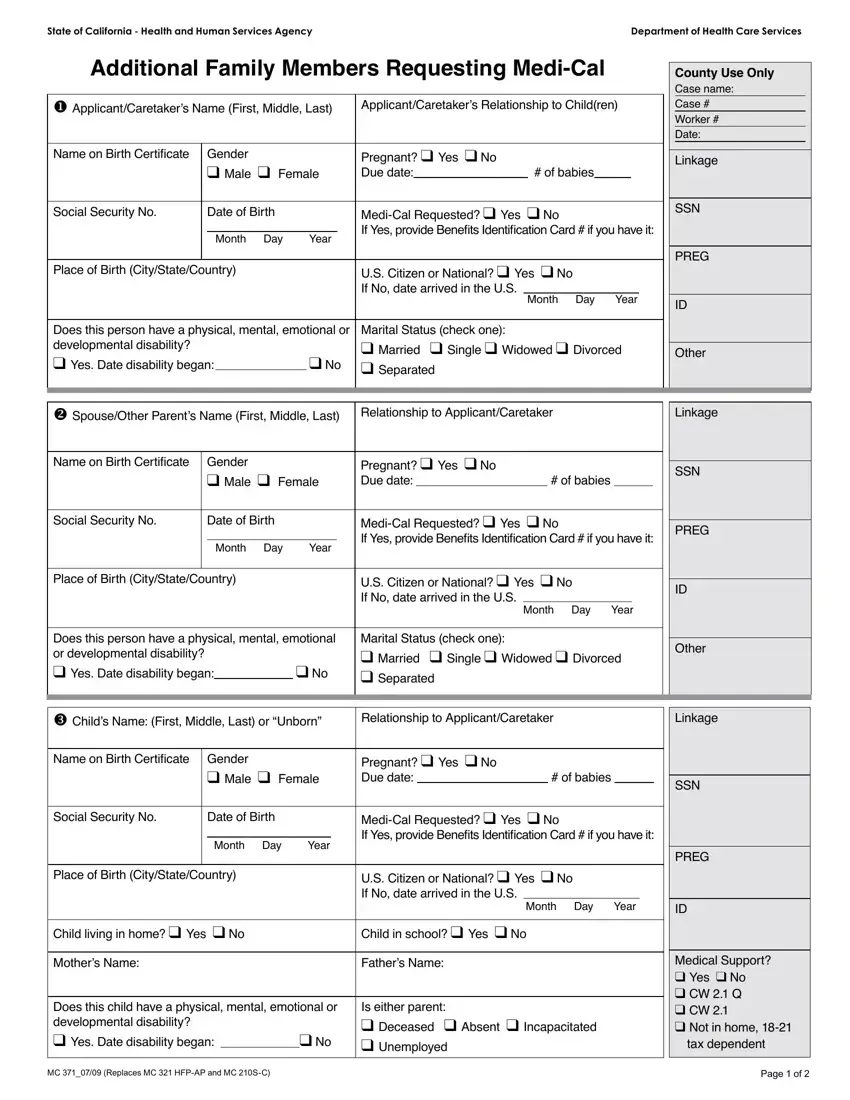
Enrolling in Medi-Cal, California's Medicaid program, involves a variety of steps and documentation to ensure that all eligible family members receive the healthcare coverage they need. Among these various forms, the MC 371 operates as a crucial document for families looking to add additional members to their Medi-Cal coverage. This form, tailored by the Department of Health Care Services, requires detailed information about each family member being added, including their personal details, health status, and current medical coverage situation. It meticulously covers applicant information, the relationship to the children being added, Social Security numbers, date of birth, and a myriad of other personal and sensitive data crucial for processing. The form not only captures basic demographic information but delves into the specifics such as pregnancy status, the potential need for retroactive coverage, and the presence of any disabilities, encapsulating a holistic view of the applicant's medical and social situation. Furthermore, the MC 371 form takes a comprehensive look at the family's financial situation, including income and expenses, to facilitate a thorough evaluation process. It underscores the importance of accuracy and honesty in reporting, as the information provided will determine the health services available to added family members. With such detailed requirements, the MC 371 form stands as a vital step for families seeking to ensure comprehensive health coverage through the Medi-Cal program, highlighting the nuanced and personalized approach taken by the State of California towards healthcare enrollment.
| Question | Answer |
|---|---|
| Form Name | Mc 371 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form mc 371, mc 371 instructions, additional family members, mc 371 |
