of Transportation |
EMPLOYMENT APPLICATION |
Page 1 of 3 |
Michigan Department |
|
0999D (01/07) |
Equal Opportunity Employer |
|
|
|
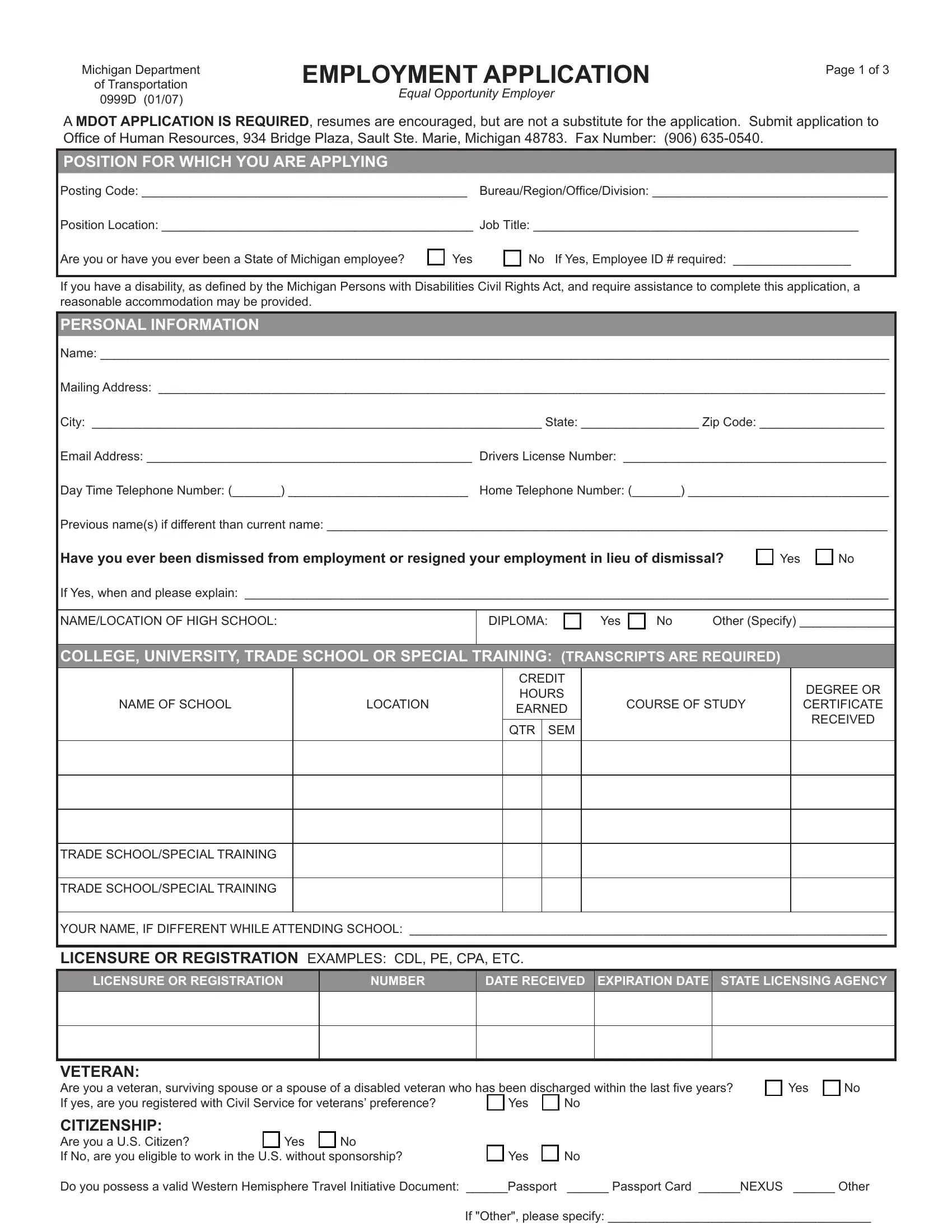
A MDOT APPLICATION IS REQUIRED, resumes are encouraged, but are not a substitute for the application. Submit application to Office of Human Resources, 934 Bridge Plaza, Sault Ste. Marie, Michigan 48783. Fax Number: (906) 635-0540.
POSITION FOR WHICH YOU ARE APPLYING
Posting Code: _______________________________________________ Bureau/Region/Office/Division: __________________________________
Position Location: _____________________________________________ JOB TITLE: _______________________________________________
Are you or have you ever been a State of Michigan employee? |
|
Yes |
|
No If Yes, Employee ID # required: _________________ |
If you have a disability, as defined by the Michigan Persons with Disabilities Civil Rights Act, and require assistance to complete this application, a reasonable accommodation may be provided.
PERSONAL INFORMATION
Name: __________________________________________________________________________________________________________________
Mailing Address: _________________________________________________________________________________________________________
City: _________________________________________________________________ State: _________________ Zip Code: __________________
Email Address: _______________________________________________ |
Drivers License Number: ______________________________________ |
Day Time Telephone Number: (_______) __________________________ |
Home Telephone Number: (_______) _____________________________ |
Previous name(s) if different than current name: _________________________________________________________________________________
Have you ever been dismissed from employment or resigned your employment in lieu of dismissal? |
Yes |
No |
If Yes, when and please explain: _____________________________________________________________________________________________
NAME/LOCATION OF HIGH SCHOOL:
No |
Other (Specify) ______________ |
COLLEGE, UNIVERSITY, TRADE SCHOOL OR SPECIAL TRAINING: (TRANSCRIPTS ARE REQUIRED)
CREDIT HOURS EARNED
QTR SEM
DEGREE OR CERTIFICATE RECEIVED
TRADE SCHOOL/SPECIAL TRAINING
TRADE SCHOOL/SPECIAL TRAINING
YOUR NAME, IF DIFFERENT WHILE ATTENDING SCHOOL: _____________________________________________________________________
LICENSURE OR REGISTRATION EXAMPLES: CDL, PE, CPA, ETC.
LICENSURE OR REGISTRATION
VETERAN:
Are you a veteran, surviving spouse or a spouse of a disabled veteran who has been discharged within the last five years? |
|
Yes |
|
No |
If yes, are you registered with Civil Service for veterans’ preference? |
|
Yes |
|
No |
|
|
|
|
CITIZENSHIP:
Are you a U.S. Citizen? |
|
Yes |
|
No |
|
|
|
|
|
If No, are you eligible to work in the U.S. without sponsorship? |
|
|
Yes |
|
No |
Do you possess a valid Western Hemisphere Travel Initiative Document: ______Passport |
______ Passport Card ______NEXUS ______ Other |
|
|
|
|
|
If "Other", please specify: ______________________________________ |
MDOT 0999D (01/07) |
Page 2 of 3 |
PERIODS OF EMPLOYMENT
Describe your work experience in detail, beginning with your current or most recent job. Include job related voluteer work, if applicable, and indicate number of employees supervised. Use a separate block to describe each position. If needed, attach additional sheets, using the same format as the application. Resumes may be attached to provide additional information.
1Name of Present or Last Employer: _______________________________________________________________________________________
Address: ___________________________________________________________________ Phone No.: (________)__________________________
Your Job Title: ________________________________________________ |
Supervisor’s Name: __________________________________________ |
FROM: _______/_______/_______ TO: _______/_______/_______ |
HOURS PER WEEK: _______ (________________________________) |
MONTH DAY |
YEAR |
MONTH DAY |
YEAR |
YOUR NAME IF DIFFERENT DURING EMPLOYMENT |
Duties and Responsibilities: _______________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
Reason for Leaving: ______________________________________________________________________________________________________________________
2Name of Present or Last Employer: _______________________________________________________________________________________
Address: ___________________________________________________________________ Phone No.: (_______)___________________________
Your Job Title: ________________________________________________ |
Supervisor’s Name: __________________________________________ |
FROM: _______/_______/_______ TO: _______/_______/_______ |
HOURS PER WEEK: _______ (________________________________) |
MONTH DAY |
YEAR |
MONTH DAY |
YEAR |
YOUR NAME IF DIFFERENT DURING EMPLOYMENT |
Duties and Responsibilities: _______________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
Reason for Leaving: ______________________________________________________________________________________________________________________
3Name of Present or Last Employer: _______________________________________________________________________________________
Address: ___________________________________________________________________ Phone No.: (________)__________________________
Your Job Title: ________________________________________________ |
Supervisor’s Name: __________________________________________ |
FROM: _______/_______/_______ TO: _______/_______/_______ |
HOURS PER WEEK: _______ (________________________________) |
MONTH DAY |
YEAR |
MONTH DAY |
YEAR |
YOUR NAME IF DIFFERENT DURING EMPLOYMENT |
Duties and Responsibilities: _______________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________
Reason for Leaving: ______________________________________________________________________________________________________________________
CERTIFICATION
I certify that all information contained in this application is true, and made in good faith. I agree and understand any falsifications, omissions, misstate- ments, or misrepresentations above will result in my forfeiting any rights of consideration for employment with the Michigan Department of Transportation or, if hired, could lead to my dismissal. Under the Michigan Persons with Disabilities Civil Rights Act, a person with a disability may allege a violation of the Act regarding the failure to accommodate only if the person with a disability notifies the employer in writing of the need for accommodation within 182 days after the date the person with a disability knew or reasonably should have known an accommodation was needed. This does not preclude my rights under federal law which establishes a 300 day status of limitation.
By submission of this application, I am authorizing the Michigan Department of Transportation to conduct a criminal history and background check, contact past employers regarding references and to check my motor vehicle operator license record as part of the pre-employment process.
SIGNATURE: ___________________________________________________________________________ DATE: _________________________
MDOT 0999D (01/07)Page 3 of 3
_EEO SURVEY |
|
|
|
|
_ |
|
|
|
|
|
Although the following information is not mandatory, it is requested to comply with Federal Highway Administration (FHWA) require- |
_ |
|
|
|
|
|
ments. This information is for statistical purposes only. It will in no way affect your employment status or opportunities, nor will it be |
_ |
|
|
|
|
|
used as part of the selection process (hiring managers will not receive this information). |
___Posting Code: _______________________________________________ |
Bureau/Region/Office/Division: __________________________________ |
__Position: ___________________________________________________ |
Location of Position___________________________________________ |
____ |
|
MALE |
|
FEMALE |
|
GENDER: |
|
|
|
____ |
|
|
|
|
|
DISABLED: |
|
NO |
|
YES |
|
__ |
|
|
|
|
|
process._ __
__ selection_ __
the__ to__
prior_ __ section_ __
this__
remove__ __
Employer,__
_
__ _ _
RACE/ETHNICITY (Please select all that apply to you):
American Indian or Alaska Native: A person having origins in any of the original peoples of North and South America (including Central America).
Asian: A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent including for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam.
Black: (not of HISpanic origin): A person having origins in any of the black racial groups.
Hispanic or Latino: A person of Mexican, Puerto Rican, Cuban, Central or South American, or other Spanish origin.
Native Hawaiian or Other Pacific Islander: A person having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands.
White (not of Hispanic origin): A person having origins in any of the original peoples of Europe, North Africa, or Middle East.
Multiracial: A person having origins in more than one racial group.