
You could complete missed punch form effortlessly using our PDFinity® online PDF tool. We are aimed at providing you the perfect experience with our editor by continuously releasing new capabilities and enhancements. Our tool has become a lot more helpful with the newest updates! At this point, filling out PDF files is a lot easier and faster than ever. For anyone who is looking to start, this is what it requires:
Step 1: Access the PDF doc in our editor by pressing the "Get Form Button" at the top of this page.
Step 2: With the help of our online PDF editor, it's possible to accomplish more than just fill out forms. Express yourself and make your forms seem faultless with customized textual content added in, or tweak the original content to excellence - all that comes with an ability to add stunning images and sign it off.
This document will require you to enter specific information; in order to guarantee correctness, be sure to take heed of the following tips:
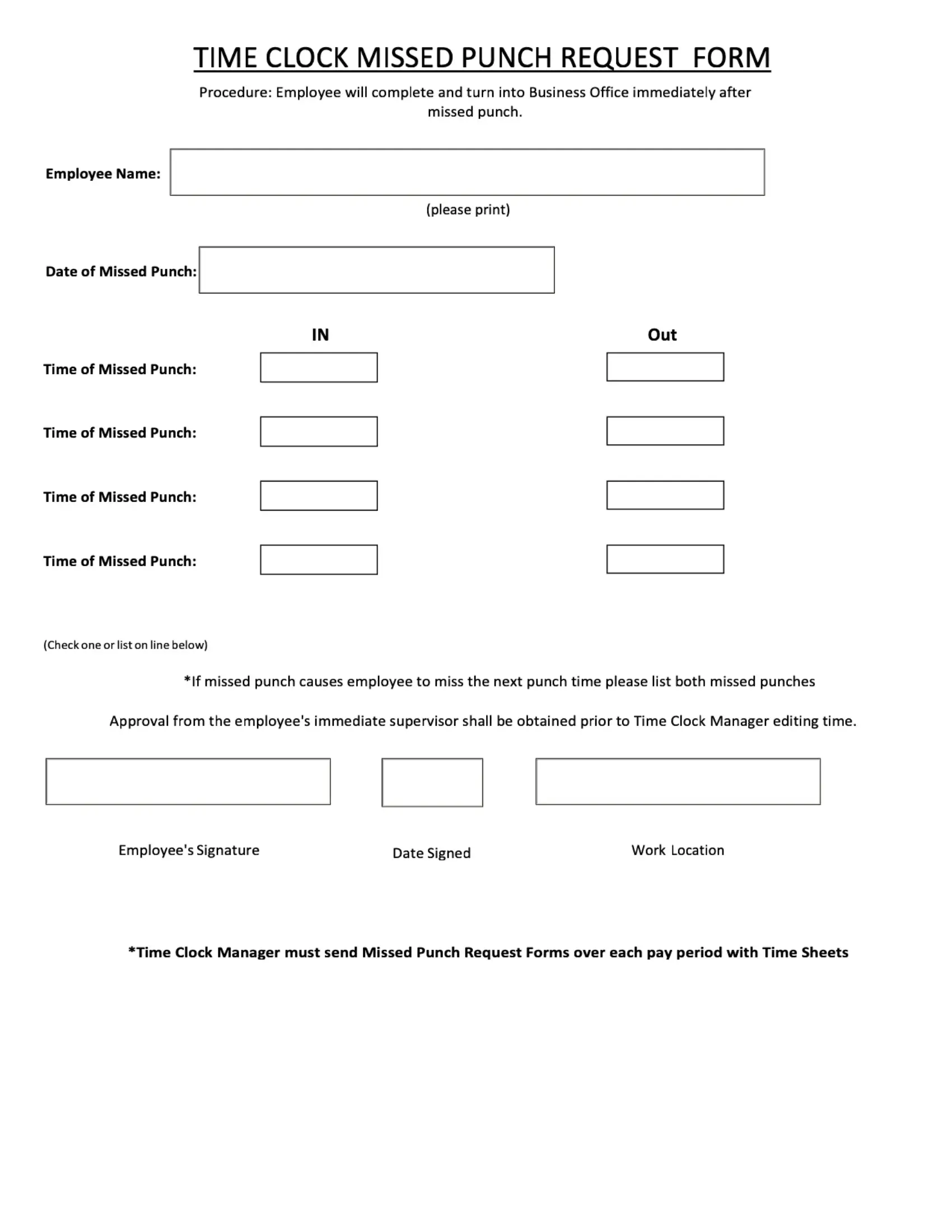
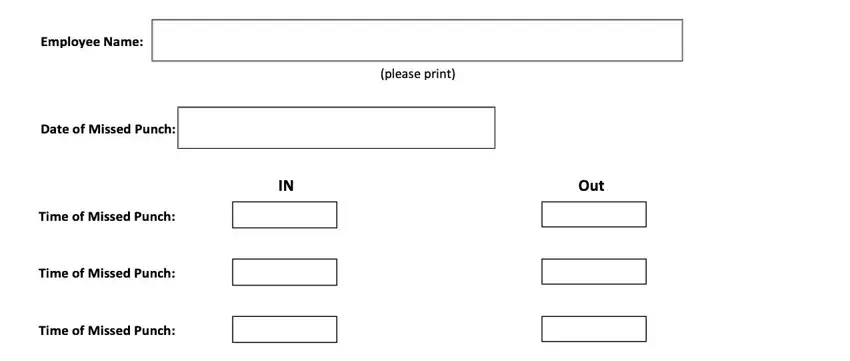
1. It is important to fill out the missed punch form properly, therefore be attentive when working with the sections containing these blanks:
2. After filling out the last step, go on to the subsequent stage and enter all required particulars in all these fields - .
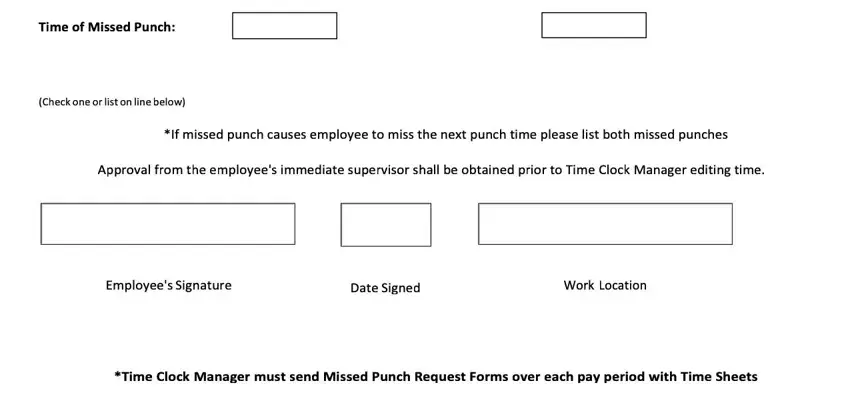
Be extremely attentive when filling in this field and next field, as this is the section where most users make errors.
Step 3: Right after double-checking the fields you've filled in, hit "Done" and you're all set! Go for a 7-day free trial account with us and obtain direct access to missed punch form - download, email, or change from your personal account. FormsPal is focused on the personal privacy of all our users; we always make sure that all information put into our system continues to be secure.