
Using PDF forms online is certainly surprisingly easy with our PDF editor. You can fill in missouri death certificates here and try out several other functions we provide. Our tool is consistently evolving to give the very best user experience achievable, and that's because of our commitment to constant improvement and listening closely to user comments. By taking a few basic steps, you are able to start your PDF editing:
Step 1: Just click on the "Get Form Button" at the top of this page to start up our pdf form editing tool. This way, you'll find everything that is required to fill out your file.
Step 2: This tool enables you to customize your PDF document in various ways. Improve it by writing any text, adjust original content, and put in a signature - all within the reach of a couple of mouse clicks!
Pay close attention when completing this document. Make sure all required blank fields are done correctly.
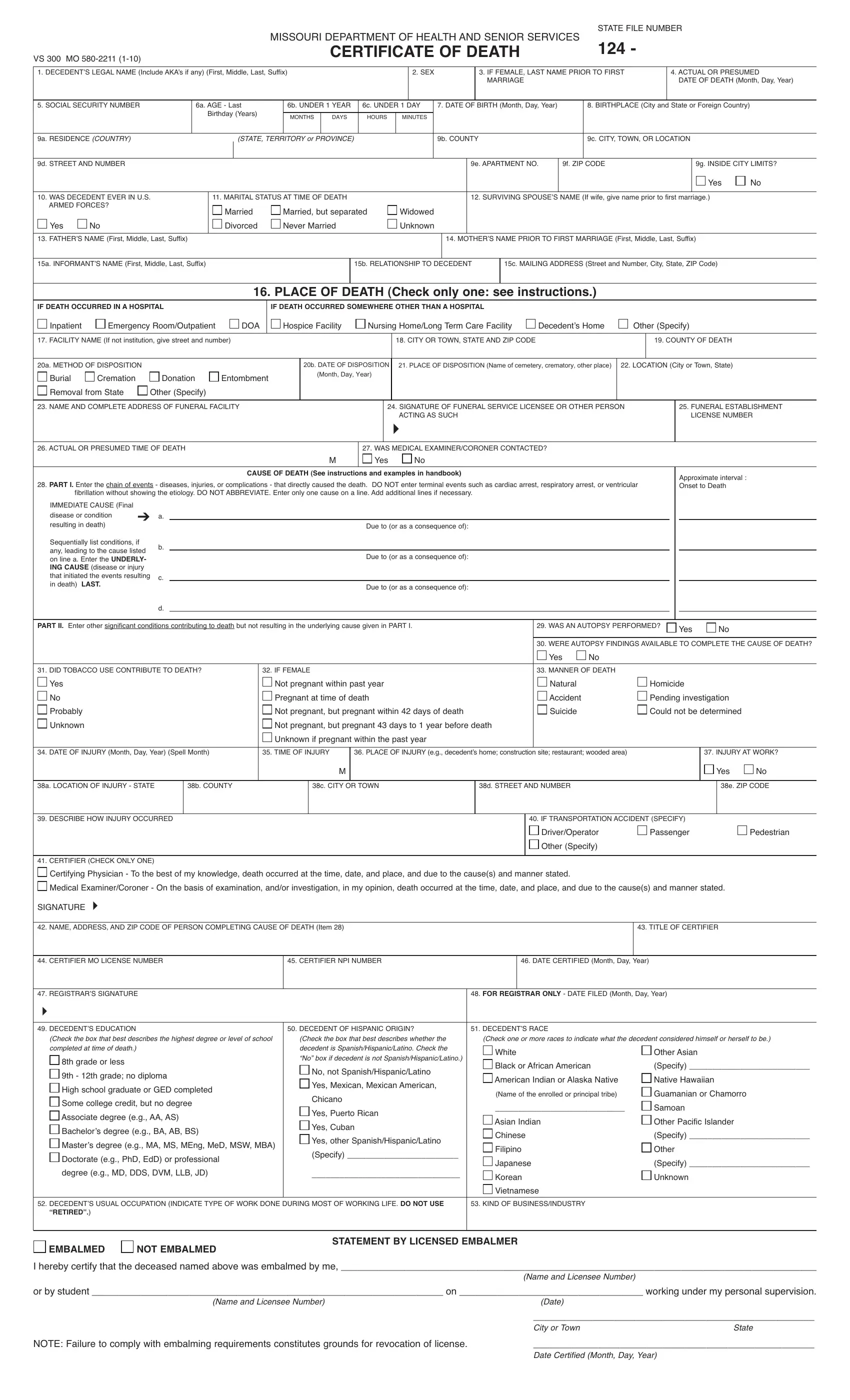
1. While filling in the missouri death certificates, make certain to complete all of the needed blanks within its relevant section. It will help hasten the work, which allows your information to be processed quickly and accurately.
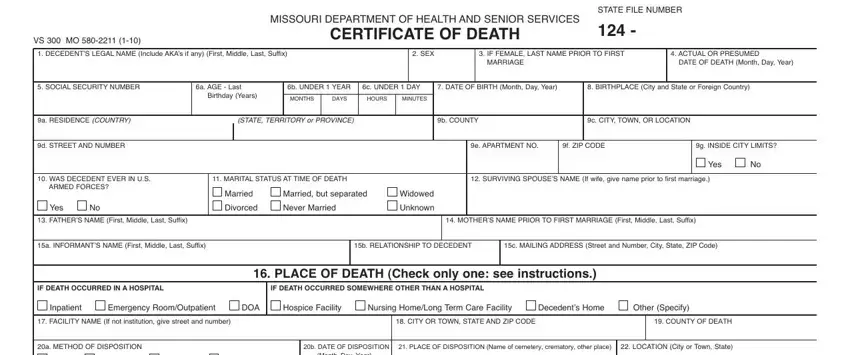
2. After this part is filled out, go on to type in the applicable information in these - Burial, Cremation, Donation, Entombment, b DATE OF DISPOSITION Month Day, Removal from State, Other Specify, NAME AND COMPLETE ADDRESS OF, ACTING AS SUCH, SIGNATURE OF FUNERAL SERVICE, FUNERAL ESTABLISHMENT, LICENSE NUMBER, ACTUAL OR PRESUMED TIME OF DEATH, WAS MEDICAL EXAMINERCORONER, and CAUSE OF DEATH See instructions.
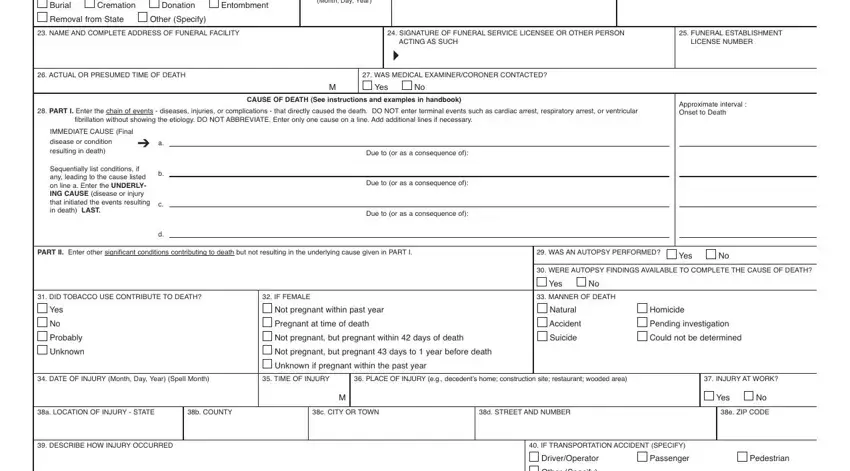
3. The next section should also be rather simple, Other Specify, CERTIFIER CHECK ONLY ONE, Certifying Physician To the best, Medical ExaminerCoroner On the, SIGNATURE, NAME ADDRESS AND ZIP CODE OF, TITLE OF CERTIFIER, CERTIFIER MO LICENSE NUMBER, CERTIFIER NPI NUMBER, DATE CERTIFIED Month Day Year, REGISTRARS SIGNATURE, FOR REGISTRAR ONLY DATE FILED, DECEDENTS EDUCATION, DECEDENT OF HISPANIC ORIGIN, and DECEDENTS RACE - all of these blanks must be completed here.
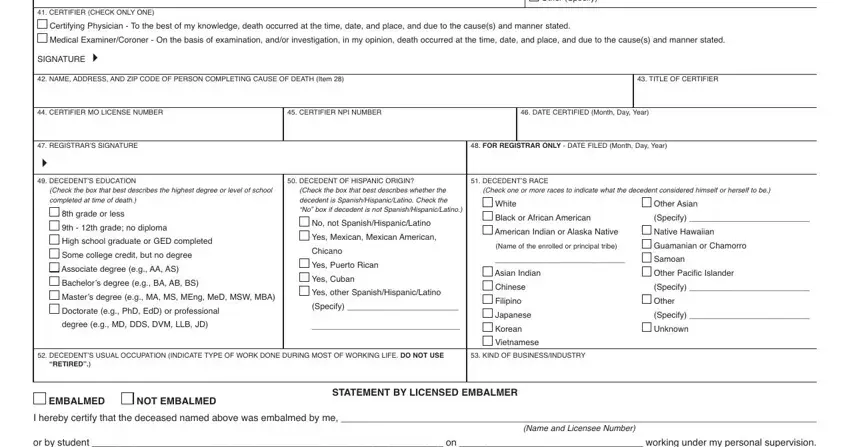
As for CERTIFIER NPI NUMBER and DECEDENTS RACE, be sure you review things in this section. Those two could be the most significant fields in the PDF.
4. All set to start working on the next section! Here you will have these or by student on working under, Name and Licensee Number, Date, NOTE Failure to comply with, City or Town, State, and Date Certified Month Day Year form blanks to do.

Step 3: Prior to finalizing this form, you should make sure that blanks were filled out the proper way. As soon as you establish that it is fine, press “Done." Obtain the missouri death certificates once you register online for a free trial. Readily gain access to the pdf file in your personal cabinet, together with any modifications and changes being all synced! FormsPal is invested in the personal privacy of all our users; we make sure all personal information entered into our tool stays protected.