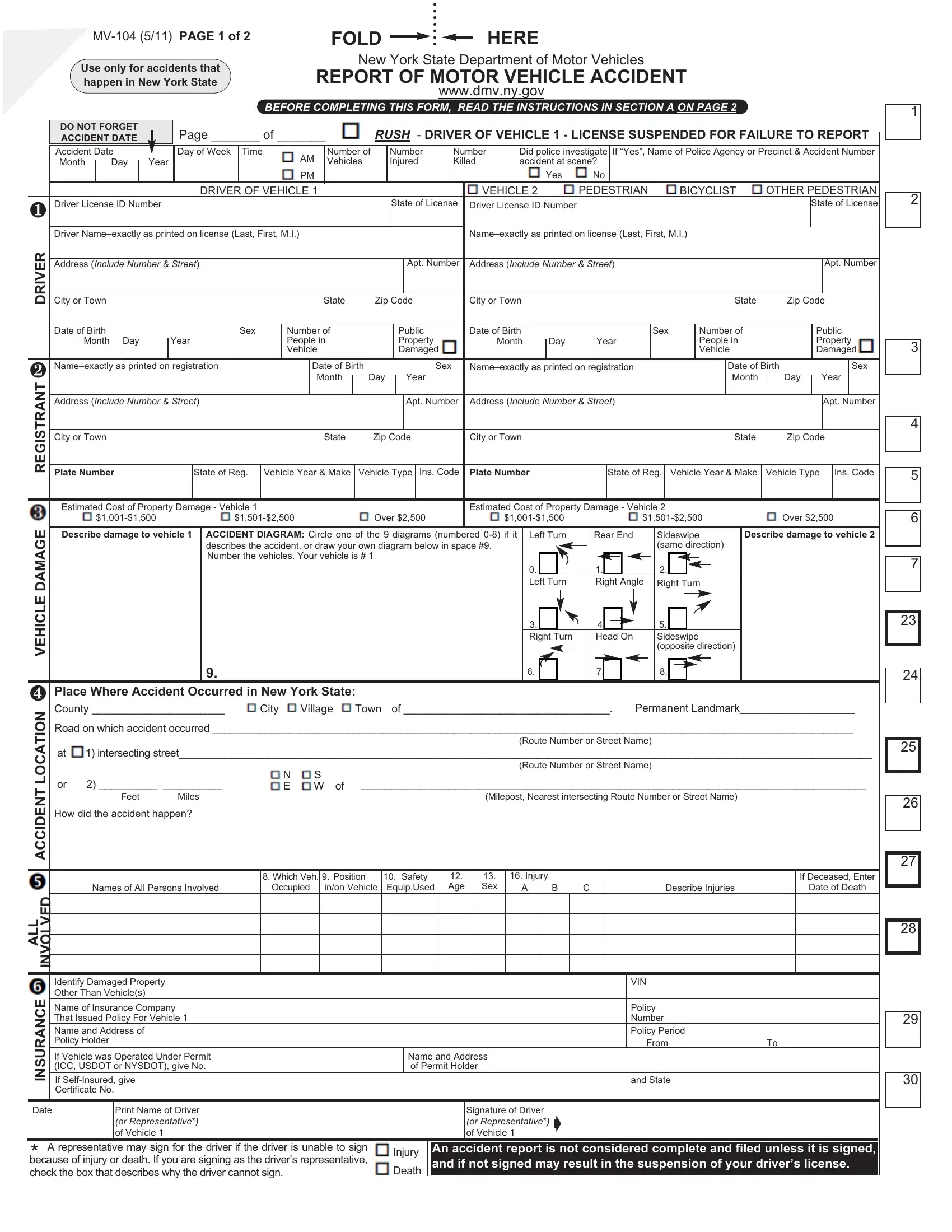

The MV-104 NY Report Accident Form must be completed accurately and submitted promptly to ensure compliance with state laws and facilitate the processing of insurance claims.
1. Determine If You Need to Report
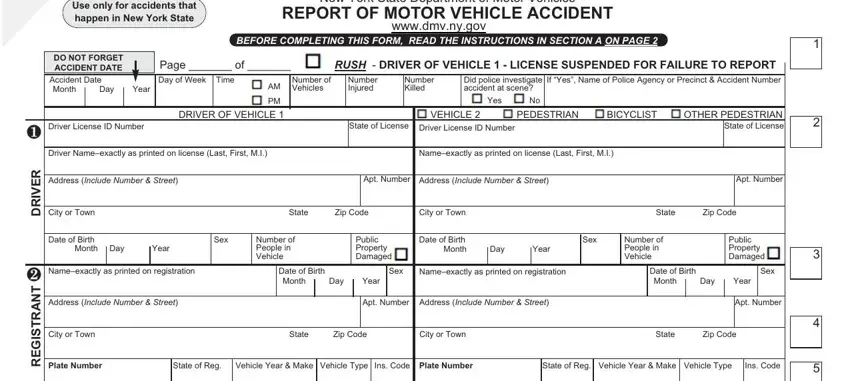
Verify whether the accident meets the criteria for reporting to the DMV, which includes any incident with personal injury, fatality, or significant property damage. This step is crucial as failing to report such accidents can lead to legal penalties.
2. Collect Necessary Information
Gather all relevant information from the accident scene, including details of all vehicles and drivers involved, insurance information, and a precise description of the accident location and conditions.
3. Document Accident Details
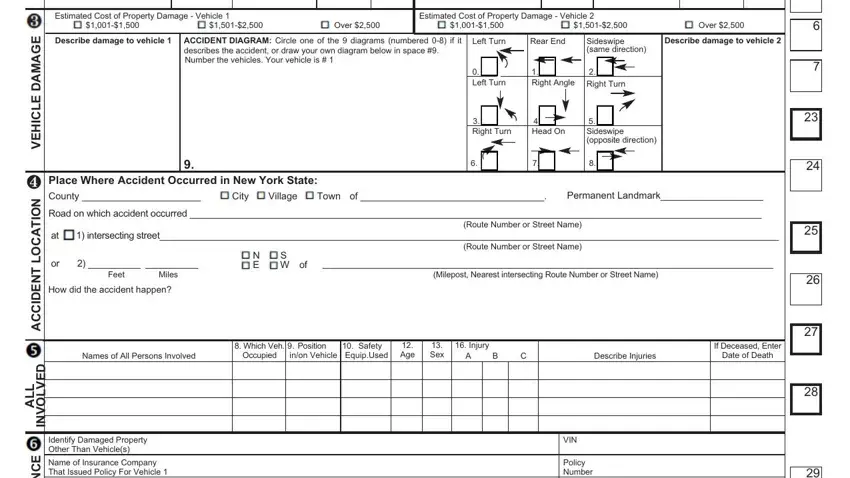
Fill in the accident date, time, and location on the form. Provide detailed descriptions, including the street names, intersections, and any landmarks to pinpoint the exact location of the accident.
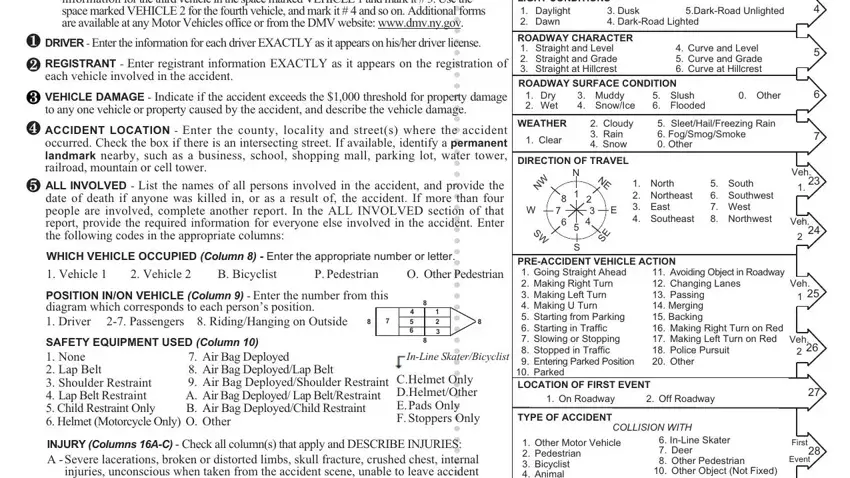
4. Fill in Driver and Vehicle Information
Enter complete driver information for each vehicle involved in the accident, including driver's license numbers, addresses, and vehicle descriptions. Make sure to include license plate numbers and insurance details.
5. Describe the Accident
Provide a detailed account of how the accident occurred in the section provided. Include all drivers' actions leading up to the accident and any contributing environmental factors.
6. Diagram the Accident
Utilize the diagram section to represent the accident's dynamics visually. This should include the positions of the vehicles at the time of the accident and their movements during the incident.
7. Report Damage and Injuries
List all damages to the vehicles and other property, and describe the nature and extent of injuries sustained by any individuals involved. Be precise in estimating the cost of damage and detailing the injuries.
8. Verify Insurance Information
Double-check that all insurance information provided is accurate and complete. This includes the insurance company name, policy number, and the period the policy covers.
9. Review and Sign the Form
Carefully review the entire form to ensure all information is correct and complete. Sign and date the form to verify the accuracy of the information provided. When you use FormsPal, you can easily fill out forms without the need to worry about personal data incidents or records getting distributed. Our protected platform makes sure that your personal information is maintained safely.