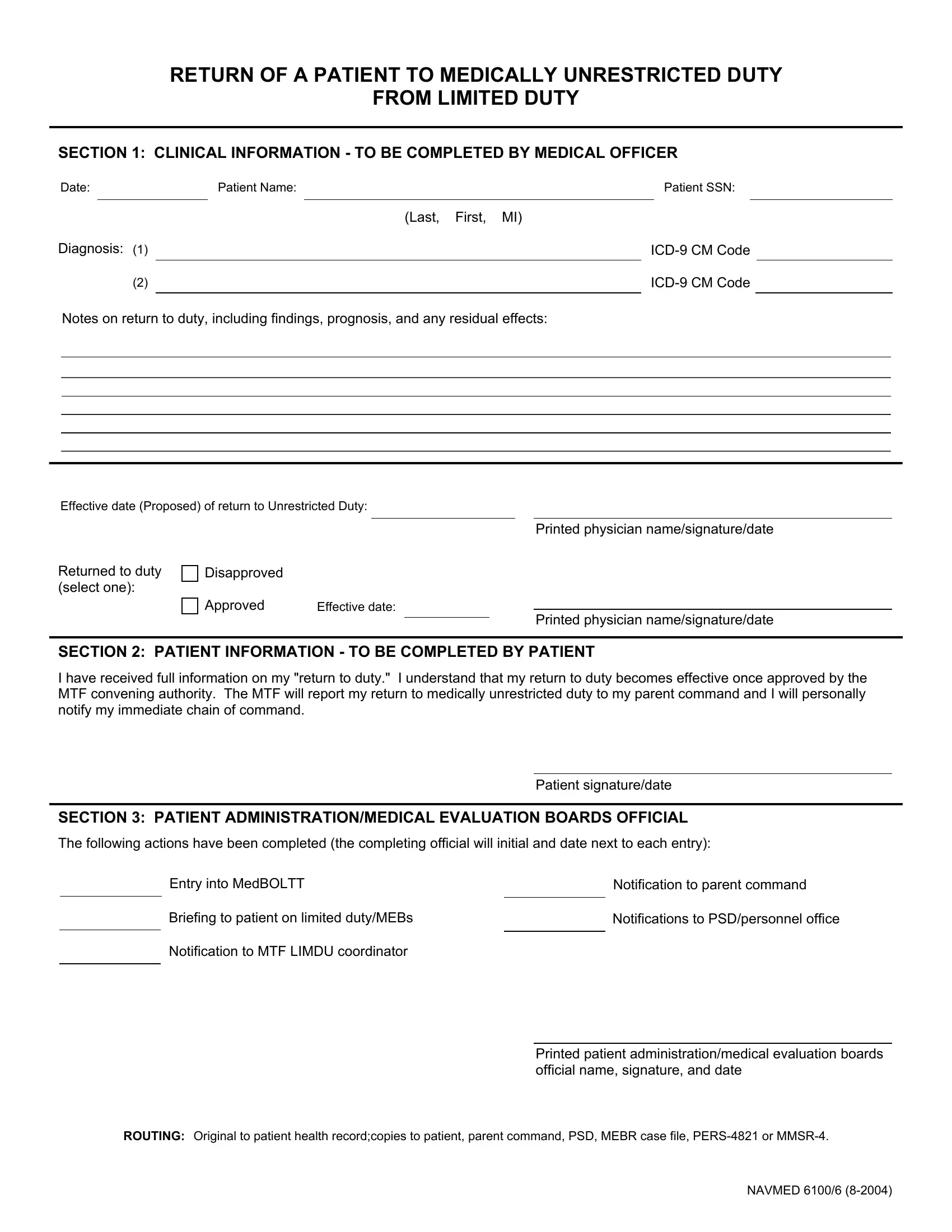
When individuals serving in various capacities reach a point where their physical condition temporarily prevents them from performing their duties without restrictions, the process for their return to full duty is both crucial and meticulously documented. This is where the NAVMED 6100/6 form plays an integral role. Primarily focused on ensuring a smooth and well-informed transition from limited to medically unrestricted duty, this form encompasses a comprehensive procedure starting with a detailed clinical assessment by a medical officer. The assessment includes the patient's name, social security number, diagnosis with ICD-9 CM codes, notes on the return to duty, including findings, prognosis, and any residual effects, followed by a section that requires the patient's acknowledgment of understanding their return to duty status. Additionally, it outlines the roles of patient administration and Medical Evaluation Boards officials in finalizing the process, covering entries into medical operational data systems, notifications to relevant commands, and briefings. The form acts as a bridge between medical evaluations and administrative actions, ensuring that both the individual and the respective commands are well-informed of the status change, making it an essential document in the realm of military healthcare administration.
| Question | Answer |
|---|---|
| Form Name | Navmed 6100 6 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 6100 6, dod 61006 duty limited form, navy navmed 61006 form, dod navmed 6100 unrestricted duty |
RETURN OF A PATIENT TO MEDICALLY UNRESTRICTED DUTY
FROM LIMITED DUTY
SECTION 1: CLINICAL INFORMATION - TO BE COMPLETED BY MEDICAL OFFICER
Date: |
|
|
Patient Name: |
|
|
Patient SSN: |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Last, |
First, MI) |
||||
Diagnosis: |
(1) |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||
|
|
(2) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Notes on return to duty, including findings, prognosis, and any residual effects:
Effective date (Proposed) of return to Unrestricted Duty:
Printed physician name/signature/date
Returned to duty (select one):
Disapproved
Approved |
Effective date: |
Printed physician name/signature/date
SECTION 2: PATIENT INFORMATION - TO BE COMPLETED BY PATIENT
I have received full information on my "return to duty." I understand that my return to duty becomes effective once approved by the MTF convening authority. The MTF will report my return to medically unrestricted duty to my parent command and I will personally notify my immediate chain of command.
Patient signature/date
SECTION 3: PATIENT ADMINISTRATION/MEDICAL EVALUATION BOARDS OFFICIAL
The following actions have been completed (the completing official will initial and date next to each entry):
Entry into MedBOLTT |
|
Notification to parent command |
Briefing to patient on limited duty/MEBs |
|
Notifications to PSD/personnel office |
|
||
Notification to MTF LIMDU coordinator |
|
|
|
|
Printed patient administration/medical evaluation boards official name, signature, and date
ROUTING: Original to patient health record;copies to patient, parent command, PSD, MEBR case file,
NAVMED 6100/6