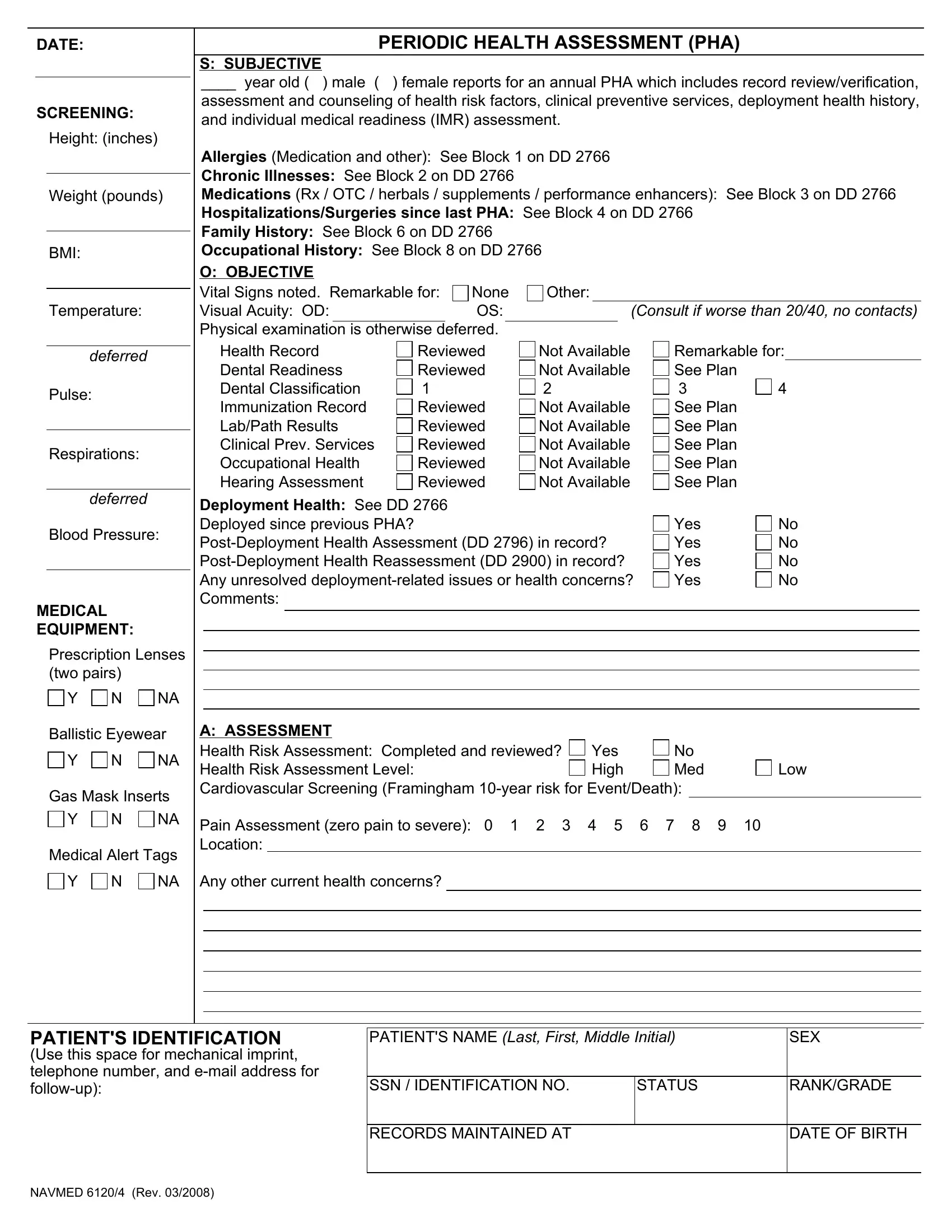
The NAVMED 6120/4 form, integral to the U.S. military's healthcare system, is a comprehensive document that plays a pivotal role in ensuring service members maintain optimum health for both deployment readiness and their overall well-being. This form facilitates the Periodic Health Assessment (PHA), a routine evaluation engrained in military protocols aimed at reviewing, assessing, and addressing the health status and risk factors present in military personnel. It meticulously accounts for various health parameters including height, weight, BMI, and vital signs, among others. The form delves into subjective details provided by the individual, such as allergies, chronic illnesses, and medication use, referencing relevant sections of the DD 2766 form for comprehensive medical history insights. Moreover, it emphasizes the importance of dental readiness, immunization records, and other clinical preventive services, ensuring a thorough scrutiny of the service member's health. Objective assessments are captured, including vision acuity and vital signs, coupled with medical equipment needs specific to deployment scenarios. The assessment portion identifies health risks and sets the stage for a personalized plan that underscores preventive measures, medical referrals, and lifestyle counseling tailored to the individual's needs. This document is not just a formality but a critical tool in sustaining the health and operational readiness of those who serve, underlining the military's commitment to its personnel's physical and mental health.
| Question | Answer |
|---|---|
| Form Name | Navmed 6120 4 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | health pha record, 6120 4, periodical health assessment, navmed 6120 |