
When you want to fill out professional complain, it's not necessary to install any kind of software - simply try using our PDF tool. The editor is continually maintained by our team, getting cool features and turning out to be more convenient. Getting underway is effortless! Everything you should do is adhere to the following basic steps directly below:
Step 1: Click the "Get Form" button above on this webpage to access our PDF editor.
Step 2: As you open the tool, there'll be the document all set to be filled in. Apart from filling in different fields, it's also possible to do other actions with the Document, including putting on your own text, modifying the original textual content, inserting illustrations or photos, placing your signature to the form, and a lot more.
Concentrate when filling in this form. Make sure all necessary blanks are done correctly.
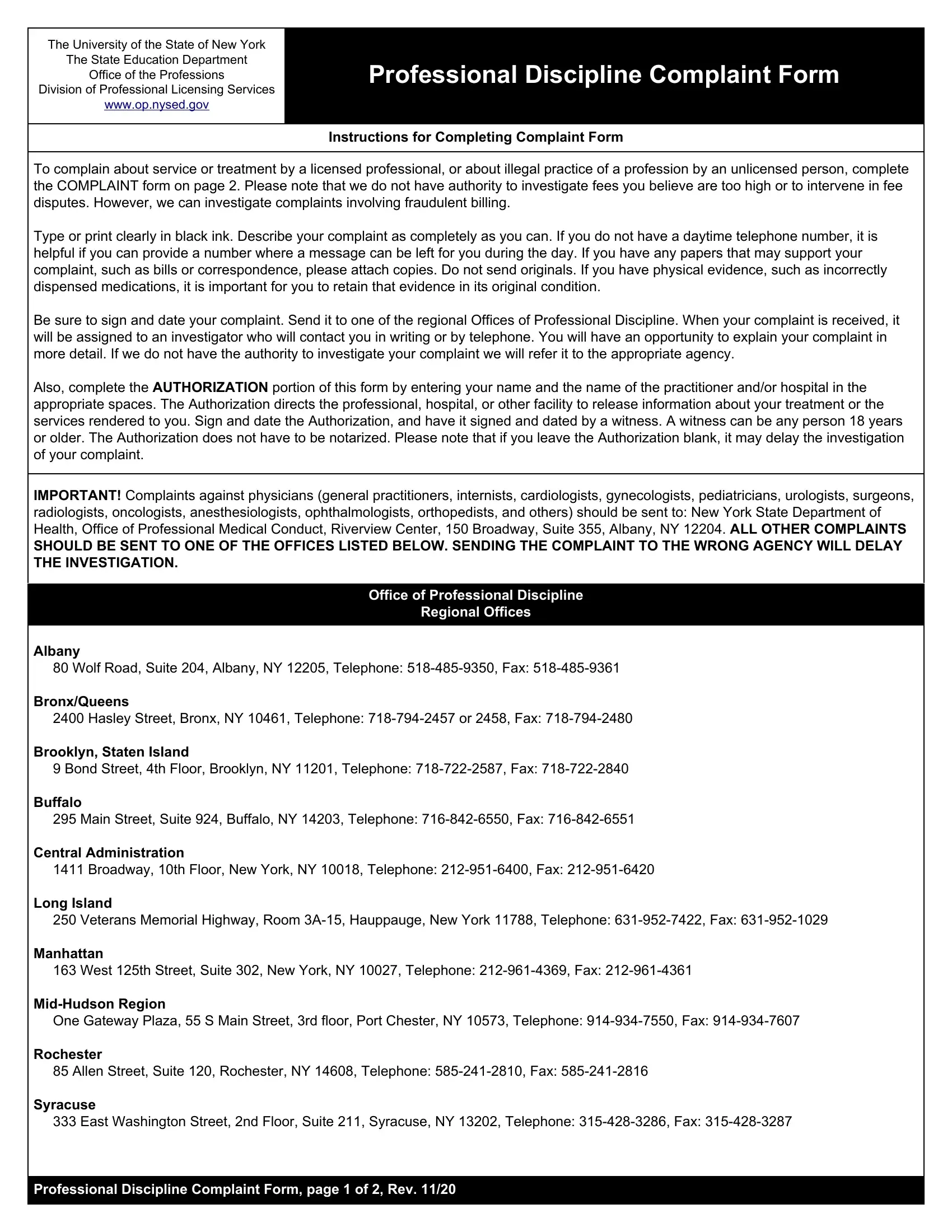
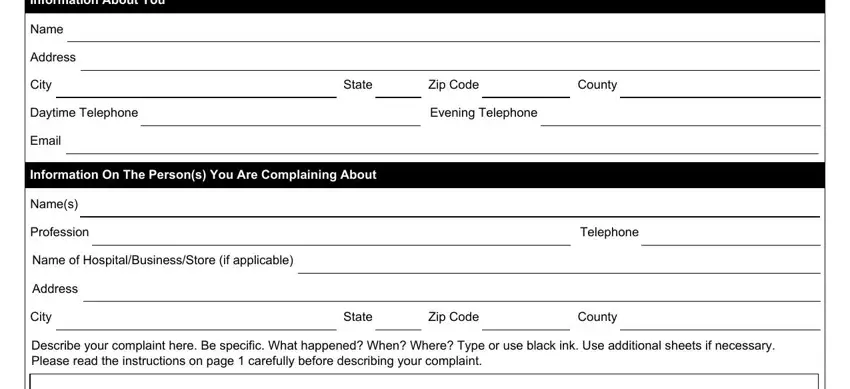
1. Fill out your professional complain with a group of necessary fields. Consider all of the required information and make sure absolutely nothing is left out!
2. Once the last segment is completed, you should insert the essential details in To the best of my knowledge the, Date, Check here if you have included, I print your name here request, Name of practitioners, Name of hospitals or other, Your Signature, Signature of witness, Date, Date, and Professional Discipline Complaint so that you can move forward to the 3rd part.
People who use this PDF frequently make some mistakes when filling in Name of hospitals or other in this part. You should definitely read again everything you enter right here.
Step 3: Ensure that your information is correct and press "Done" to progress further. Try a 7-day free trial option with us and get direct access to professional complain - with all adjustments saved and accessible inside your personal account. At FormsPal, we do our utmost to be certain that all of your details are maintained private.