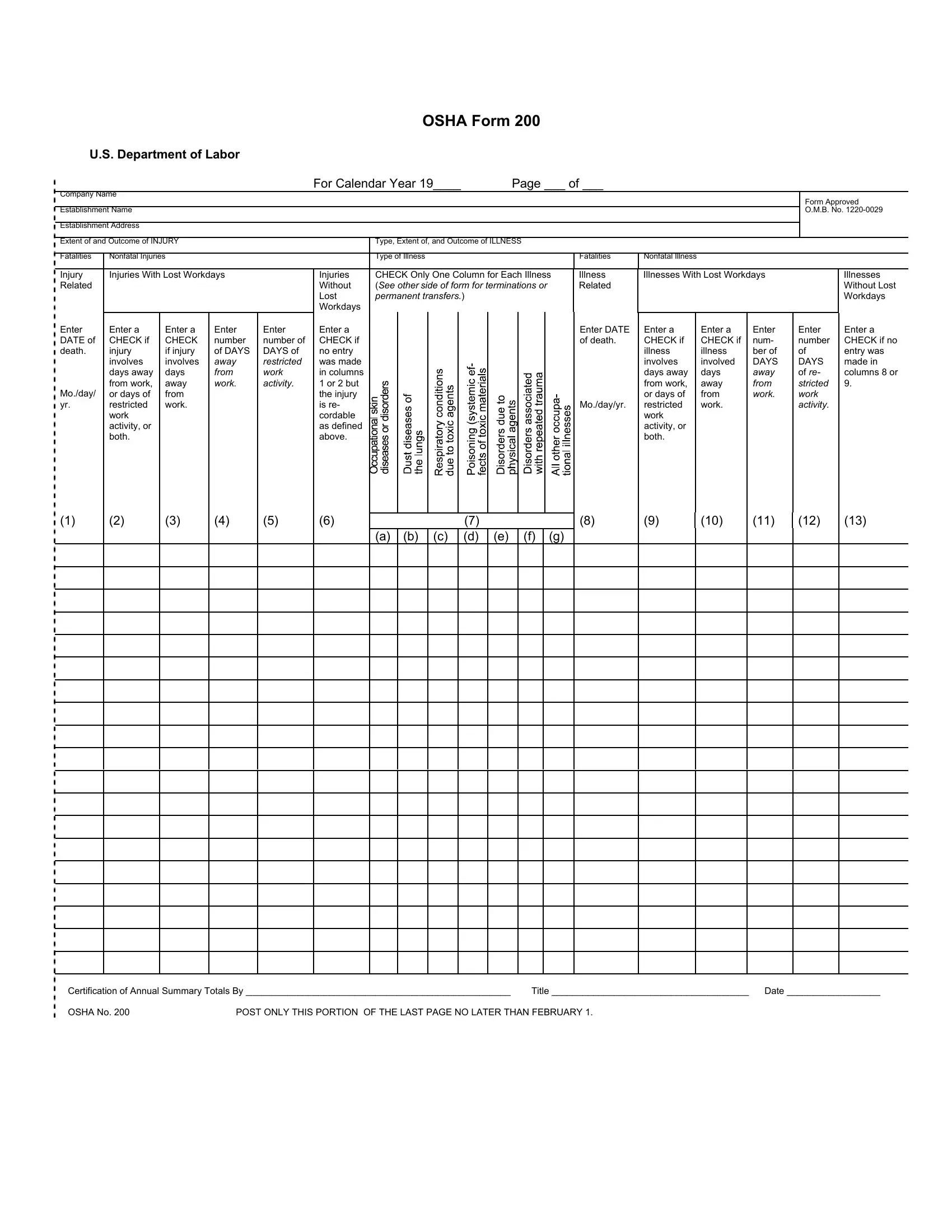
The OSHA Form 200, endorsed by the U.S. Department of Labor, operates as a crucial tool in the realm of occupational safety and health documentation for the calendar year it covers. At its core, the form serves as a comprehensive log and summary of occupational injuries and illnesses, which businesses are mandated to maintain and post within their establishments. This record-keeping not only aids in monitoring workplace safety incidents but also plays a vital role in the formulation of preventive measures against future occurrences. It meticulously categorizes incidents into injuries and illnesses, delineating between fatal and nonfatal outcomes, and further specifies cases involving lost workdays. Moreover, this form demands detailed entry of each incident, including the date, employee details, a description of the injury or illness alongside its extent, and the outcome. By requiring information about days away from work or days of restricted activity, it facilitates an in-depth analysis of the impact of workplace incidents. The obligation to complete and publicly post the summary of this form by a set deadline underscores the importance of transparency and accountability in upholding workplace safety. With penalties for noncompliance, the OSHA Form 200 exemplifies a rigorous approach towards ensuring that occupational health standards are not just met but continuously improved upon.
| Question | Answer |
|---|---|
| Form Name | Osha 200 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | osha log 200 form, osha form 200 log, osha form 200, osha 200 logs |
