INSTRUCTIONS FOR USE OF FORM OWCP-915
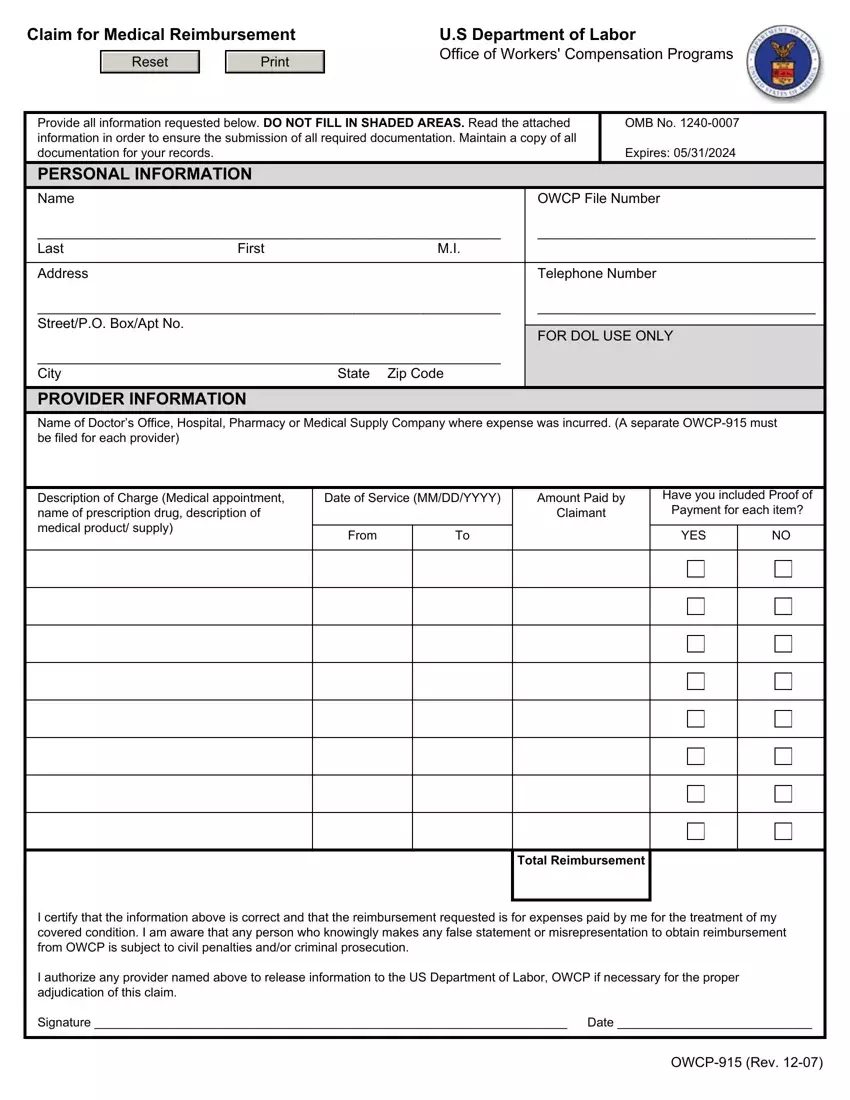
•This form is to be used to seek reimbursement for out of pocket medical expenses pertaining to the treatment of an accepted condition. Form OWCP-915 can be used to seek reimbursement for expenses in regard to medical treatment, prescription medication and medical supplies.
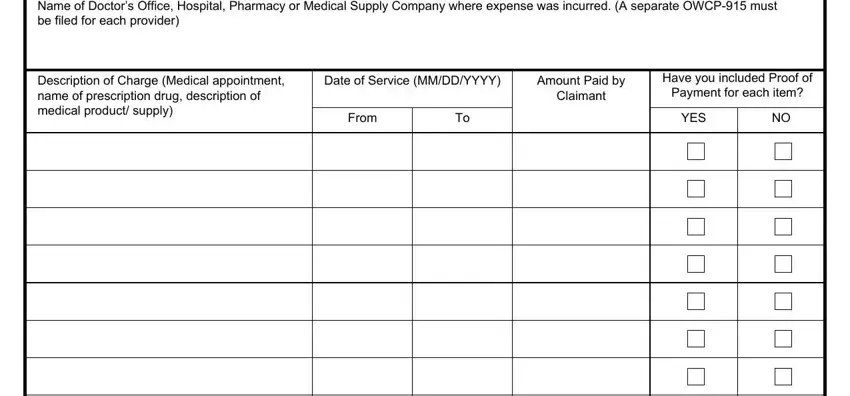
•Please submit a separate reimbursement claim for each provider where an out of pocket expense was incurred.
•Please print clearly and legibly. Reference your OWCP file number on all documentation. Maintain a copy of the completed OWCP- 915 and supporting documentation for your records.
DOCUMENTATION REQUIRED FOR MEDICAL REIMBURSEMENT
Prescription Medication
1.Completed OWCP-915
2.A paper pharmacy billingform, which must be attached to the OWCP-915 and must include the following information:
a.Name, address and telephone number of pharmacy
b.Pharmacy provider number
c.Prescription number
d.Name of claimant
e.Date of purchase
f.Eleven Digit National Drug Code (NDC#)
g.New prescription or refill number
h.Quantity of medication (e.g. # of pills or ml/cc)
i.Amount paid by employee per medication
3.Proof of payment (can include cash receipt, cancelled check or credit card slip)
Medical Expense other than prescription medication
1.Completed OWCP-915
2.Physicians and other health care providers (i.e. physical therapists) must complete Form OWCP-1500. Hospitals and other facilities, such as ambulatory surgical centers, skilled nursing facilities, etc. must submit their bills on Form OWCP-04. Every form must be completed in its entirety in the same manner as bills submitted by the provider directly to OWCP. The amount paid by the claimant must be indicated. The OWCP-1500 or OWCP-04 must be attached to this form. It is the responsibility of the person submitting
a claim for reimbursement to obtain a completed OWCP-1500 or OWCP-04 from the provider rendering service. Without a fully completed OWCP-1500 or OWCP-04, the OWCP is not able to process a reimbursement.
3.Proof of payment (can include cash receipt, cancelled check or credit card slip)
Travel
Do not use Form OWCP-915 to submit a claim for travel reimbursement. Claims for travel reimbursement should be submitted on Form OWCP-957.
Public Burden Statement
Public reporting burden for this collection of information is estimated to average 10 minutes per response, including time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. If you have any comments regarding the burden estimate or any other aspect to this collection of information, including suggestions for reducing this burden, send them to the Office of Workers’ Compensation Programs, U.S. Department of Labor, Room S3524, 200 Constitution Avenue, N.W., Washington, D.C. 20210. Do not submit the completed claim form to this address. Persons are not required to respond to this information collection unless it displays a currently valid OMB number.