
form pa 635 or 1663 can be filled in online without difficulty. Simply use FormsPal PDF tool to accomplish the job quickly. To keep our tool on the cutting edge of practicality, we strive to put into practice user-driven features and improvements regularly. We're routinely grateful for any suggestions - assist us with reshaping how you work with PDF files. This is what you would want to do to get going:
Step 1: Simply click the "Get Form Button" at the top of this webpage to start up our pdf form editing tool. There you will find everything that is necessary to fill out your file.
Step 2: Using this online PDF editor, you are able to do more than simply fill in forms. Edit away and make your docs look perfect with custom textual content put in, or modify the file's original content to perfection - all that backed up by an ability to add your own photos and sign the document off.
This document will need some specific information; to ensure accuracy, please be sure to pay attention to the suggestions listed below:
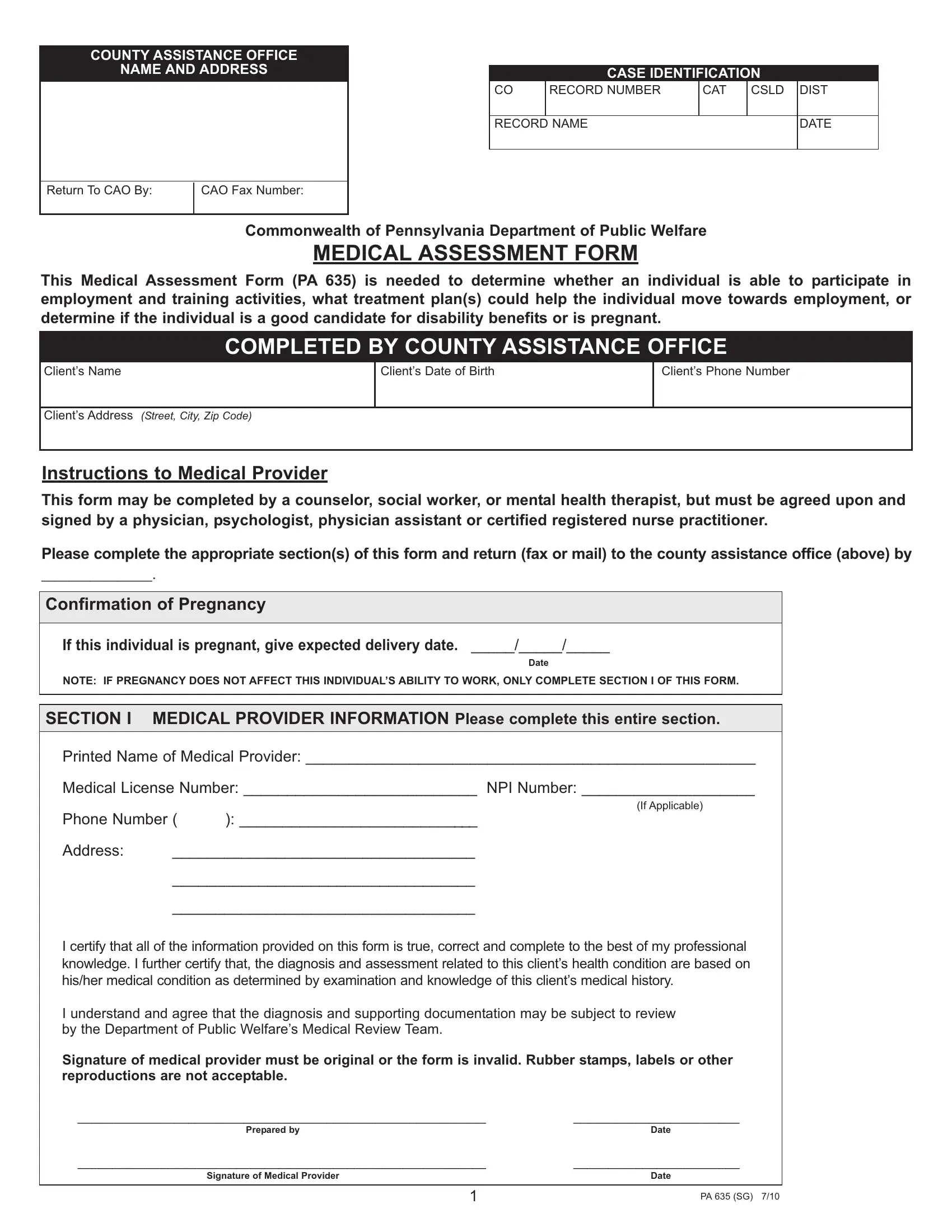
1. The form pa 635 or 1663 involves certain details to be inserted. Make sure the following blanks are completed:
2. The third stage is usually to complete the following fields: Please complete the appropriate, Confirmation of Pregnancy, If this individual is pregnant, Date, NOTE IF PREGNANCY DOES NOT AFFECT, SECTION I MEDICAL PROVIDER, Printed Name of Medical Provider, Medical License Number NPI Number, If Applicable, Phone Number, Address, and I certify that all of the.
3. Completing Signature of medical provider must, Prepared by, Date, Signature of Medical Provider, Date, and PA SG is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

4. Filling out CountyRecord Number, Clients Name, Date of Birth, SECTION II EMPLOYABILITY, IF CHECKBOX IS SELECTED FOR THIS, IF EMPLOYABLE THIS INDIVIDUAL WILL, EMPLOYABLE, This individual is able to work or, with the following reasonable, LIMITED EMPLOYABILITY Please, This individual is able to work or, see above Approximately how many, With the following reasonable, What is the recommended treatment, and basis for the hours that are is crucial in this next section - make sure to be patient and be attentive with each field!
5. The last stage to conclude this PDF form is pivotal. You need to fill out the required fields, such as basis for the hours that are, Prescribed Medication Therapy, Referral Made for Patient, Other describe, This individual is expected to be, sustained basis until, Date, TEMPORARY INCAPACITY Please, This individuals physical or, sustained basis at this time but, This individuals temporary, Date, What is the recommended treatment, basis for the hours that are, and Prescribed Medication Therapy, before submitting. Failing to accomplish that can end up in a flawed and potentially nonvalid document!
Those who work with this PDF frequently make some errors when filling out This individuals temporary in this section. You should definitely read twice whatever you enter here.
Step 3: Always make sure that the details are accurate and then just click "Done" to continue further. Make a 7-day free trial account with us and obtain immediate access to form pa 635 or 1663 - which you'll be able to then use as you would like from your FormsPal cabinet. Here at FormsPal.com, we aim to be certain that your details are stored secure.