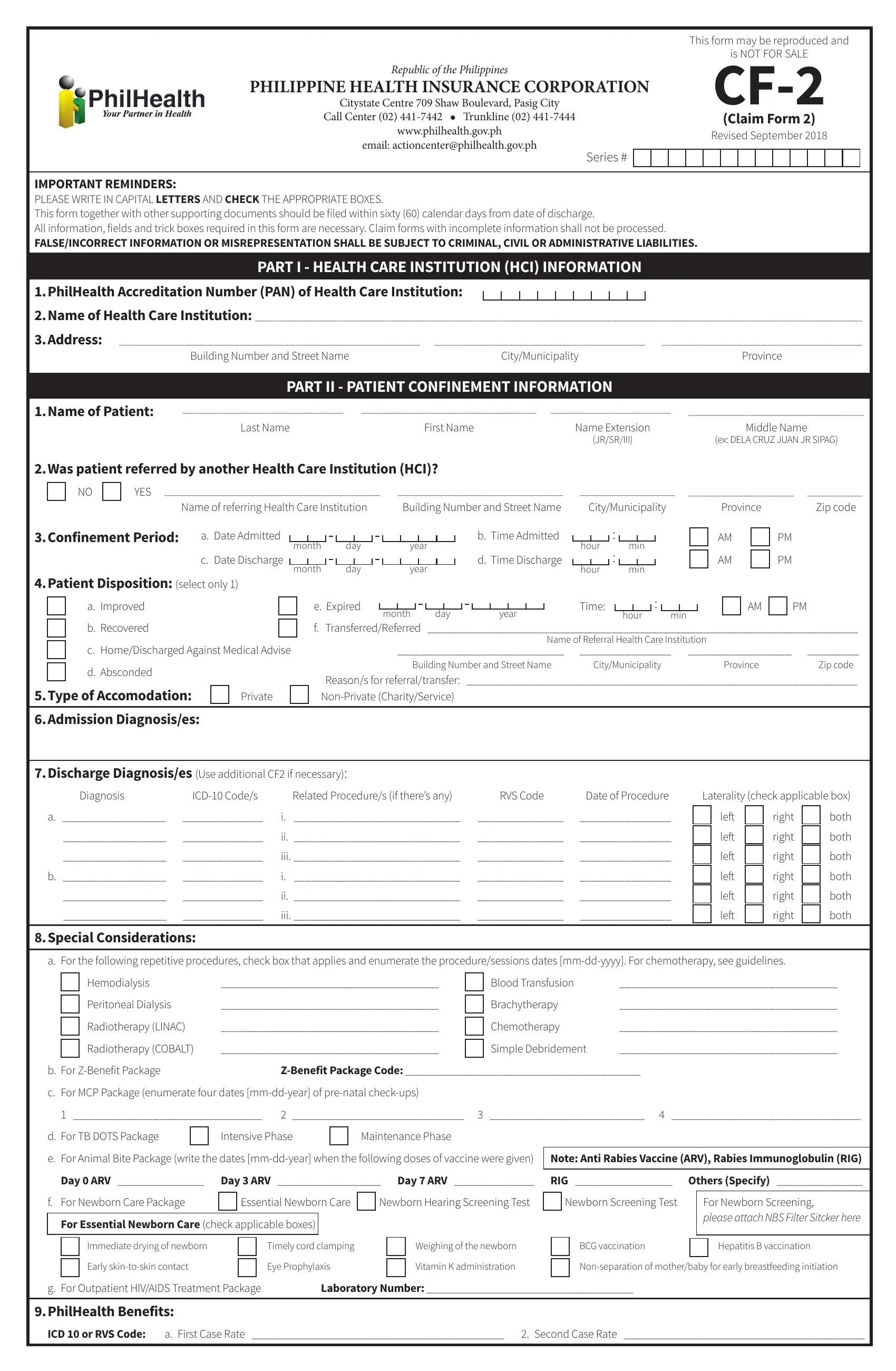
In the realm of social health insurance in the Philippines, the PhilHealth CF2 form stands as a crucial document for processing medical claims and ensuring that beneficiaries receive the appropriate healthcare coverage. This form, officially a release by the Philippine Health Insurance Corporation, is part of a streamlined process designed to provide clarity and ease in settling medical claims. As indicated on the document, it may be reproduced and is explicitly not for sale, emphasizing its accessibility and utility for all Filipinos covered under the PhilHealth program. The form, last revised in September 2018, requires submission within a strict timeframe of sixty calendar days following the patient's date of discharge, underscoring the importance of timely filing. It encompasses detailed sections, including health care institution information, patient confinement details, diagnoses, and a certification of the consumption of benefits, each meticulously designed to capture comprehensive data pertinent to the claim. Instructions stress the importance of writing in capital letters and checking the appropriate boxes, with an admonition that incomplete information will lead to processing delays. Moreover, the form includes strict reminders against false or incorrect information which could result in criminal, civil, or administrative liabilities, thus upholding the integrity of the submission process. Importantly, it accommodates details not only on the diagnosis and treatment received but also supports the inclusion of special considerations such as the Z-Benefit Package and procedures like chemotherapy or hemodialysis, further illustrating the form's adaptability to various patient needs.
| Question | Answer |
|---|---|
| Form Name | Philhealth CF-2 Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 222 |
| Avg. time to fill out | 22 min 29 sec |
| Other names | philhealth claim form 2, philhealth form cf2, cf2 form, csf2 form |
|
This form may be reproduced and |
|
|
is NOT FOR SALE |
|
Republic of the Philippines |
||
PHILIPPINE HEALTH INSURANCE CORPORATION |
||
Citystate Centre 709 Shaw Boulevard, Pasig City |
||
Call Center (02) |
(Claim Form 2) |
|
www.philhealth.gov.ph |
Revised September 2018 |
|
email: actioncenter@philhealth.gov.ph |
||
|
Series #
IMPORTANT REMINDERS:
PLEASE WRITE IN CAPITAL LETTERS AND CHECK THE APPROPRIATE BOXES.
This form together with other supporting documents should be filed within sixty (60) calendar days from date of discharge.
All information, fields and trick boxes required in this form are necessary. Claim forms with incomplete information shall not be processed.
FALSE/INCORRECT INFORMATION OR MISREPRESENTATION SHALL BE SUBJECT TO CRIMINAL, CIVIL OR ADMINISTRATIVE LIABILITIES.
PART I - HEALTH CARE INSTITUTION (HCI) INFORMATION
1.PhilHealth Accreditation Number (PAN) of Health Care Institution:
2.Name of Health Care Institution: _________________________________________________________________________________________________________________________
3.Address: ____________________________________________________________ __________________________________________ ________________________________________
Building Number and Street NameCity/MunicipalityProvince
PART II - PATIENT CONFINEMENT INFORMATION
1.Name of Patient: |
________________________________ |
___________________________________ |
________________________ |
___________________________________ |
|
Last Name |
First Name |
Name Extension |
Middle Name |
|
|
|
(JR/SR/III) |
(ex: DELA CRUZ JUAN JR SIPAG) |
2.Was patient referred by another Health Care Institution (HCI)?
|
|
NO |
|
YES ___________________________________________ |
_________________________________ |
||||||||||||||||||
|
|
|
|
|
Name of referring Health Care Institution |
|
|
Building Number and Street Name |
|||||||||||||||
3.Confinement Period: |
a. Date Admitted |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. Time Admitted |
||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
month |
day |
|
|
year |
||||||||||||
|
|
|
|
|
c. Date Discharge |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. Time Discharge |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
month |
day |
|
|
year |
||||||||||||
4.Patient Disposition: (select only 1)
___________________ |
_____________________ ___________ |
||||||||||||
City/Municipality |
|
|
Province |
Zip code |
|||||||||
|
|
: |
|
|
|
|
|
|
|
|
AM |
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
hour |
: |
|
min |
|
|
|
|
|
|||||
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
AM |
|
PM |
|
|
|
|
|
|
|
|
|
||||||
hour |
|
|
min |
|
|
|
|
|
|||||
|
|
|
|
|
|||||||||
|
|
a. Improved |
|
|
|
|
|
e. Expired |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time: |
|
|
|
|
|
: |
|
|
|
|
|
|
|
|
AM |
|
|
PM |
|
|
|
|
|
|
|
|
|
|
month |
|
day |
|
year |
|
|
hour |
|
|
min |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
b. Recovered |
|
|
|
|
|
f. Transferred/Referred |
___________________________________________________________________________ |
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Referral Health Care Institution |
|
||||||||||||||||||
|
|
c. Home/Discharged Against Medical Advise |
_____________________________ |
________________ |
|
|
__________________ |
_________ |
|||||||||||||||||||||||||||||||||||||||||
|
|
d. Absconded |
|
|
|
|
|
|
|
|
|
Building Number and Street Name |
City/Municipality |
|
|
|
Province |
Zip code |
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
Reason/s for referral/transfer: ____________________________________________________________________ |
||||||||||||||||||||||||||||||||||||||||||
5.Type of Accomodation: |
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
Private |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
6.Admission Diagnosis/es:
7.Discharge Diagnosis/es (Use additional CF2 if necessary):
Diagnosis |
Related Procedure/s (if there’s any) |
RVS Code |
Date of Procedure |
|
a. __________________ |
______________ |
i. _____________________________ |
_______________ |
________________ |
__________________ |
______________ |
ii. _____________________________ |
_______________ |
________________ |
__________________ |
______________ |
iii. _____________________________ |
_______________ |
________________ |
b. __________________ |
______________ |
i. _____________________________ |
_______________ |
________________ |
__________________ |
______________ |
ii. _____________________________ |
_______________ |
________________ |
__________________ |
______________ |
iii. _____________________________ |
_______________ |
________________ |
Laterality (check applicable box)
left |
|
right |
|
both |
left |
|
right |
|
both |
|
|
|||
left |
|
right |
|
both |
left |
|
right |
|
both |
|
|
|||
left |
|
right |
|
both |
left |
|
right |
|
both |
8.Special Considerations:
a. For the following repetitive procedures, check box that applies and enumerate the procedure/sessions dates
Hemodialysis |
______________________________________ |
|
Blood Transfusion |
______________________________________ |
Peritoneal Dialysis |
______________________________________ |
|
Brachytherapy |
______________________________________ |
|
||||
Radiotherapy (LINAC) |
______________________________________ |
|
Chemotherapy |
______________________________________ |
|
||||
Radiotherapy (COBALT) |
______________________________________ |
|
Simple Debridement |
______________________________________ |
|
b. For |
|
c. For MCP Package (enumerate four dates |
|
1 _________________________________ 2 ______________________________ 3 ___________________________ 4 _________________________________
d. For TB DOTS Package |
|
|
Intensive Phase |
|
|
Maintenance Phase |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
e. For Animal Bite Package (write the dates |
Note: Anti Rabies Vaccine (ARV), Rabies Immunoglobulin (RIG) |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Day 0 ARV _______________ |
|
Day 3 ARV __________________ Day 7 ARV ______________ |
RIG _________________ |
Others (Specify) _______________ |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
f. For Newborn Care Package |
|
|
Essential Newborn Care |
|
Newborn Hearing Screening Test |
|
Newborn Screening Test |
|
For Newborn Screening, |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
please attach NBS Filter Sitcker here |
For Essential Newborn Care (check applicable boxes) |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Immediate drying of newborn
Early
Timely cord clamping
Eye Prophylaxis
Weighing of the newborn
Vitamin K administration
BCG vaccination |
|
Hepatitis B vaccination |
|
|
|
g. For Outpatient HIV/AIDS Treatment Package |
Laboratory Number: ____________________________________ |
9.PhilHealth Benefits:
ICD 10 or RVS Code: |
a. First Case Rate ____________________________________________ 2. Second Case Rate __________________________________________ |
10.Accreditation Number/Name of Accredited Health Care Professional/Date Signed and Professional Fees/Charges
(Use additional CF2 if necessary):
Accreditation number/Name of Accredited Health Care Professional/Date Signed |
|
|
Details |
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accreditation No.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
____________________________________________________________ |
|
|
No |
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
Signature Over Printed Name |
|
|
With |
P |
______________________ |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Date Signed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
month |
|
day |
|
|
year |
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accreditation No.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
____________________________________________________________ |
|
|
No |
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
Signature Over Printed Name |
|
|
With |
P |
______________________ |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Date Signed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
month |
|
day |
|
|
year |
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accreditation No.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
____________________________________________________________ |
|
|
No |
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
Signature Over Printed Name |
|
|
With |
P |
______________________ |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Date Signed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
month |
|
day |
|
|
year |
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART III - CERTIFICATION OF CONSUMPTION OF BENEFITS AND CONSENT TO ACCESS PATIENT RECORD/S
NOTE: Member/Patient should sign only after the applicable charges have been
A.CERTIFICATION OF CONSUMPTION OF BENEFITS:
PhilHealth benefit is enough to cover HCI and PF Charges.
No purchase of drugs/medicines, supplies, diagnostics, and
Total Health Care Institution Fees
Total Professional Fees
Grand Total
Total Actual Charges*
The benefit of the member/patient was completely consumed prior to
a.) The total
|
|
Amount after Application |
|
|
|
|
|
|
|
Total Actual Charges* |
of Discount (i.e., personal |
|
PhilHealth Benefit |
Amount after PhilHealth Deduction |
|||
|
|
discount, Senior Citizen/PWD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Amount P _______________________ |
||
Total Health Care |
|
|
|
|
|
Paid by (check all that applies): |
||
Institution Fees |
|
|
|
|
|
Member/Patient |
HMO |
|
|
|
|
|
|
|
Others (i.e., PCSO, Promisory note, etc.) |
||
|
|
|
|
|
|
|
||
Total Professional |
|
|
|
|
|
Amount P _______________________ |
||
Fees (for accredited |
|
|
|
|
|
Paid by (check all that applies): |
||
and |
|
|
|
|
|
Member/Patient |
HMO |
|
professionals) |
|
|
|
|
|
Others (i.e., PCSO, Promisory note, etc.) |
||
|
|
|
|
|
|
|
|
|
b.) Purchases/Expenses NOT included in the Health Care Institution Charges |
|
|
|
|
|
|||
|
|
|
|
|
|
|||
Total cost of purchase/s for drugs/medicines and/or medical supplies bought by the |
|
None |
Total Amount |
P |
_______________ |
|||
patient/member within/outside the HCI during confinement |
|
|||||||
|
|
|
|
|
||||
|
|
|
|
|
|
|||
Total cost of diagnostic/laboratory examinations paid by the patient/member done |
|
None |
Total Amount |
P |
_______________ |
|||
within/outside the HCI during confinement |
|
|
|
|||||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
*NOTE: Total Actual Charges should be based on Statement of Account (SOA)
B.CONSENT TO ACCESS PATIENT RECORD/S:
I hereby consent to the submission and examination of the patient’s pertinent medical records for the purpose of verifying the veracity of this claim to effect efficient processing of benefit payment.
I hereby hold PhilHealth or any of its officers, employees and/or representatives free from any and all legal liabilities relative to the
_____________________________________________________________
Signature Over Printed Name of Member/Patient/Authorized Representative
Date Signed:
month |
day |
year |
|
Relationship of the representative to |
Spouse |
Child |
Parent |
the member/patient: |
Sibling |
Others, Specify ___________________ |
|
Reason for signing on behalf of the |
Patient is Incapacitated |
|
|
member/patient: |
Other Reasons _______________________________ |
||
If patient/representative is unable to write, put right thumbmark. Patient/ Representative should be assisted by an HCI representative.
Patient
Representative
PART IV - CERTIFICATION OF CONSUMPTION OF HEALTH CARE INSTITUTION
I certify that services rendered were recorded in the patient’s chart and health care institution records and that the herein information given are true and correct.
____________________________________________________ |
__________________________________________ |
Date Signed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Signature Over Printed Name of Authorized HCI Representative |
Official Capacity/Designation |
|
|
month |
day |
year |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||