
We've used the efforts of the best software engineers to create the PDF editor you are going to work with. The application will allow you to create the sf 2823 designations form effortlessly and don’t waste valuable time. All you need to undertake is keep up with these quick tips.
Step 1: Press the button "Get form here" to get into it.
Step 2: You can now alter the sf 2823 designations. The multifunctional toolbar permits you to include, delete, improve, and highlight content material or undertake other commands.
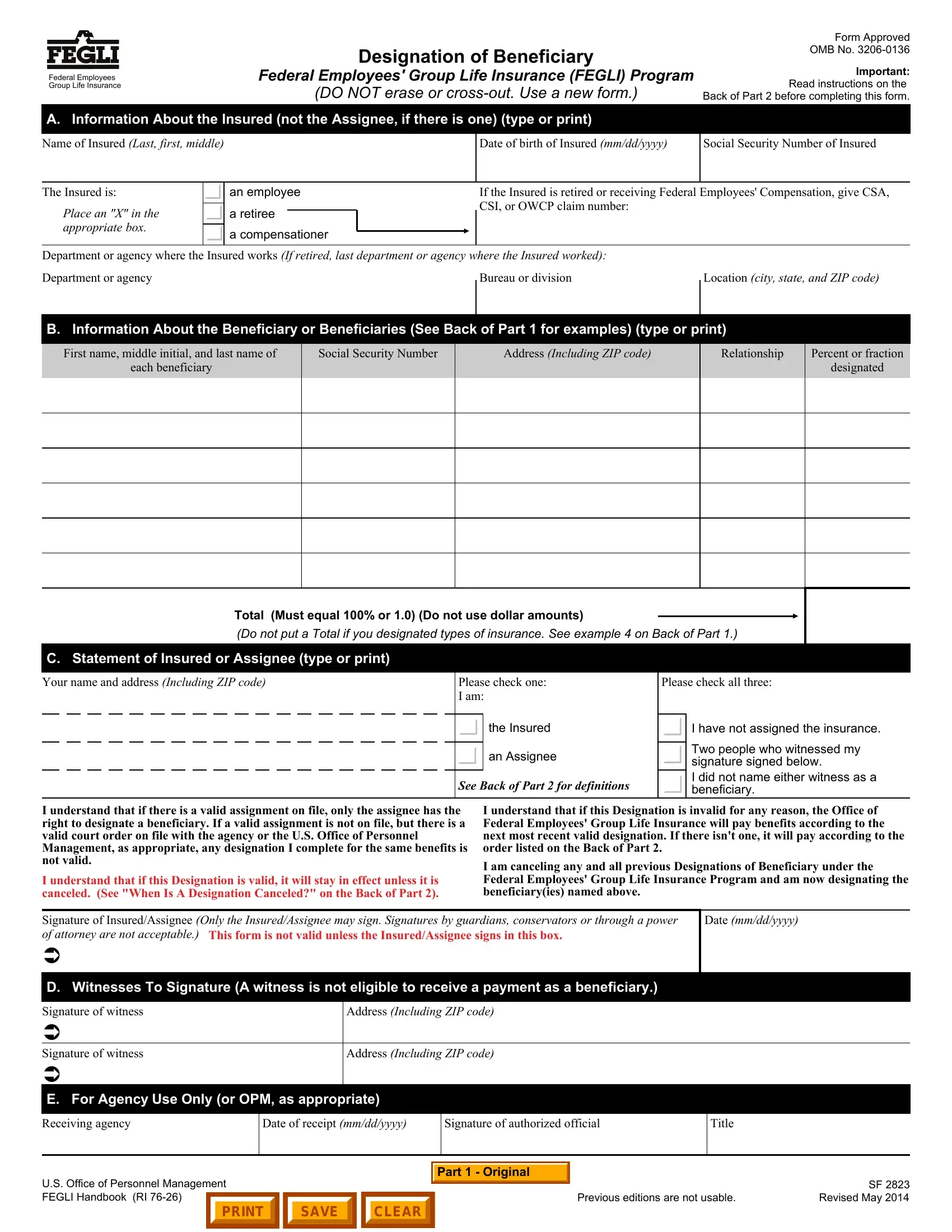
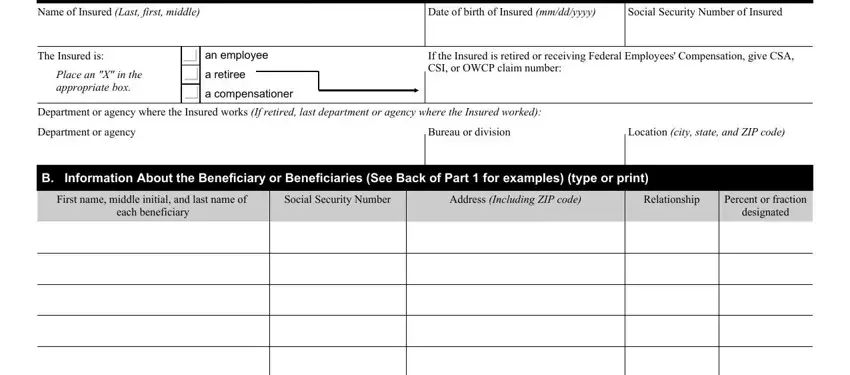
In order to prepare the sf 2823 designations PDF, provide the information for each of the sections:
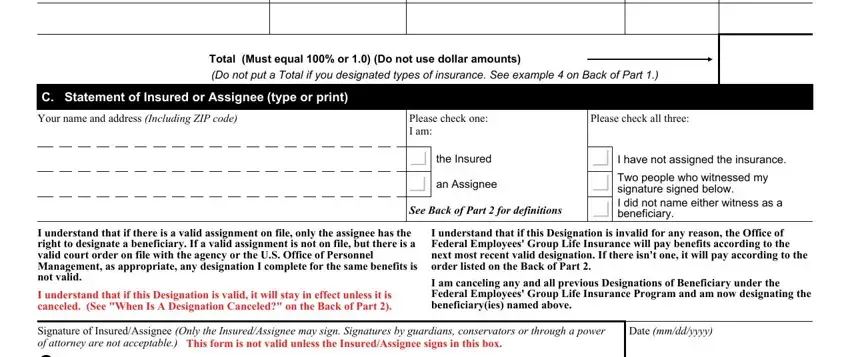
You should enter the required details in the Total Must equal or Do not use, C Statement of Insured or Assignee, Your name and address Including, Please check one I am, the Insured, an Assignee, See Back of Part for definitions, Please check all three, I have not assigned the insurance, Two people who witnessed my, I understand that if there is a, I understand that if this, I understand that if this, I am canceling any and all, and Signature of InsuredAssignee Only area.
You will have to note particular particulars inside the area US Office of Personnel Management, Previous editions are not usable, and SF Revised May.

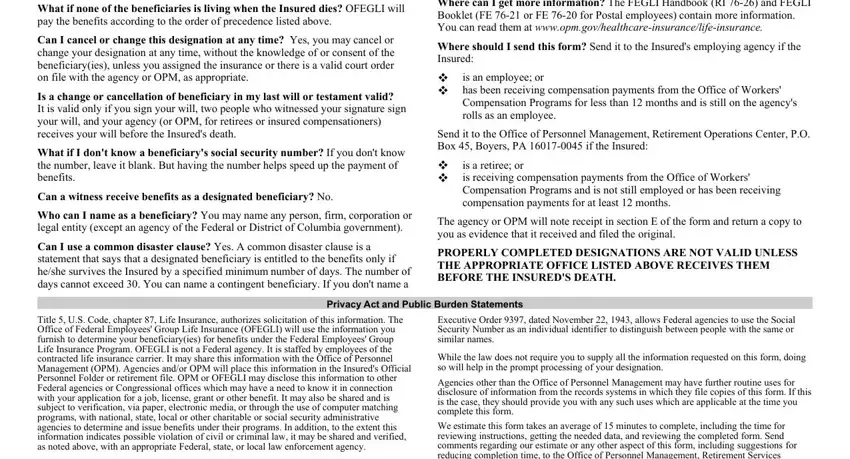
Please make sure to write down the rights and obligations of the sides inside the What if none of the beneficiaries, Can I cancel or change this, Is a change or cancellation of, What if I dont know a beneficiarys, Can a witness receive benefits as, Who can I name as a beneficiary, Can I use a common disaster clause, Where can I get more information, Where should I send this form Send, is an employee or has been, Send it to the Office of Personnel, is a retiree or is receiving, The agency or OPM will note, PROPERLY COMPLETED DESIGNATIONS, and Privacy Act and Public Burden section.
Step 3: Select the button "Done". The PDF document is available to be transferred. You can save it to your laptop or send it by email.
Step 4: In order to avoid possible upcoming risks, make certain you have more than a few copies of every single file.