Our PDF editor makes managing files simple and easy. It is rather easy to update the [FORMNAME] document. Check out all of these actions in an attempt to do it:
Step 1: Choose the orange "Get Form Now" button on the following page.
Step 2: You're now on the document editing page. You may edit, add information, highlight certain words or phrases, insert crosses or checks, and add images.
The next areas are in the PDF document you'll be filling out.
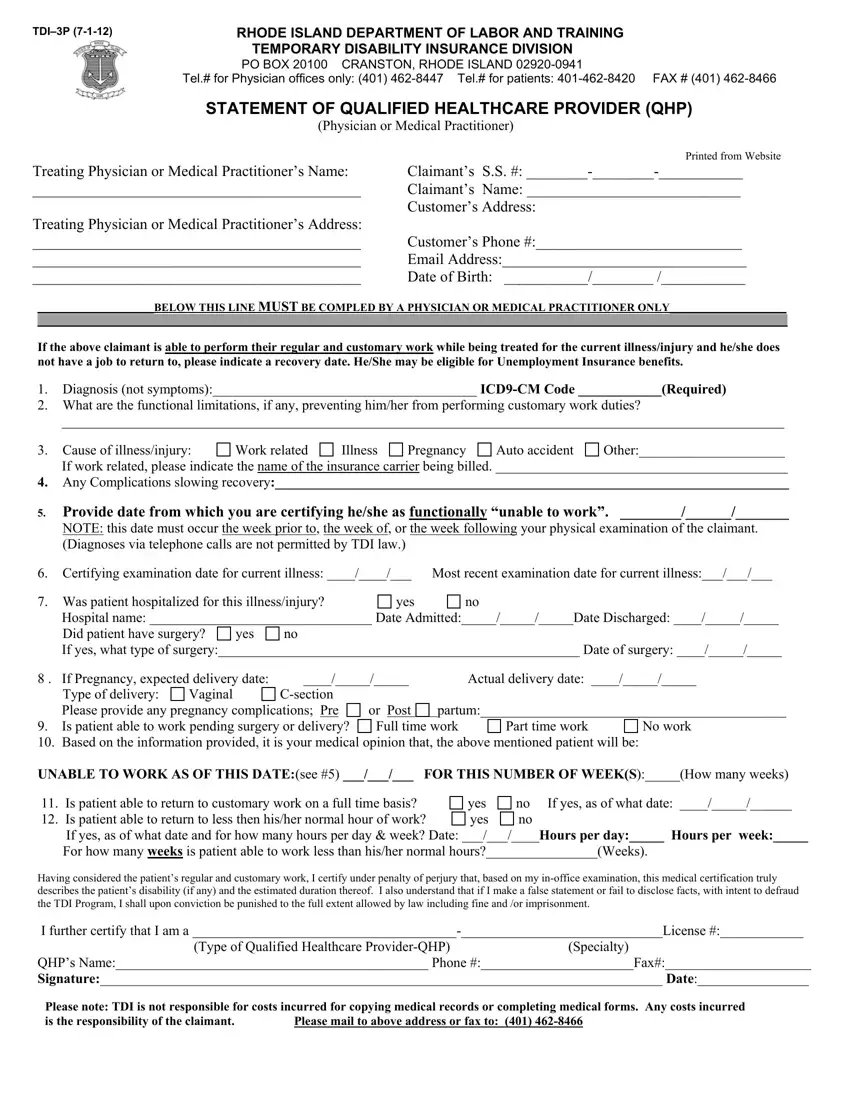
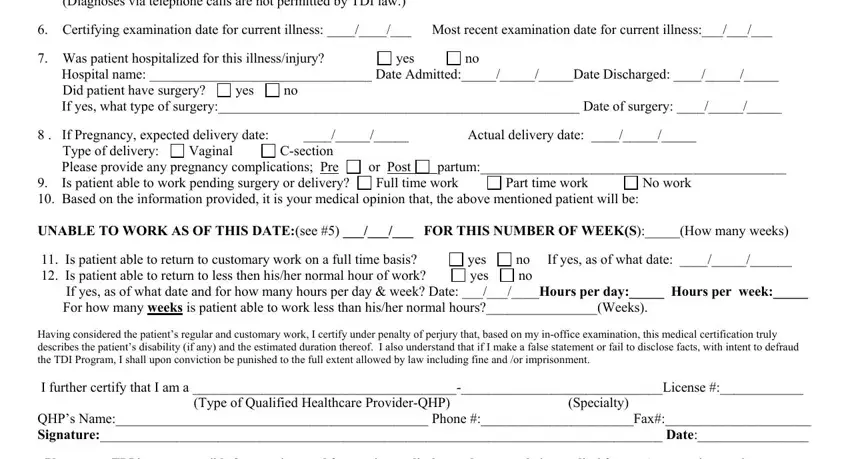
Include the demanded particulars in the Provide date from which you are, Certifying examination date for, Was patient hospitalized for this, yes, Did patient have surgery, yes, If yes what type of surgery Date, If Pregnancy expected delivery, Type of delivery, Vaginal, Csection, Please provide any pregnancy, Part time work, Full time work, and or Post part.
Step 3: If you are done, choose the "Done" button to export your PDF document.
Step 4: To avoid potential forthcoming difficulties, you need to possess minimally two or three copies of each separate form.
