









You can easily create the bank pet insurance form form using this PDF editor. The following steps will help you quickly prepare your document.
Step 1: Select the orange "Get Form Now" button on the web page.
Step 2: At this point, you can start editing your bank pet insurance form. The multifunctional toolbar is available to you - insert, erase, change, highlight, and undertake several other commands with the text in the file.
Prepare the bank pet insurance form PDF by entering the content necessary for each individual section.
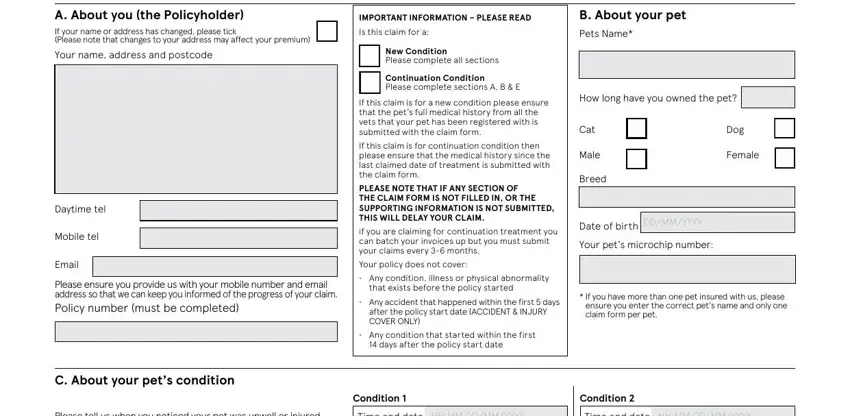
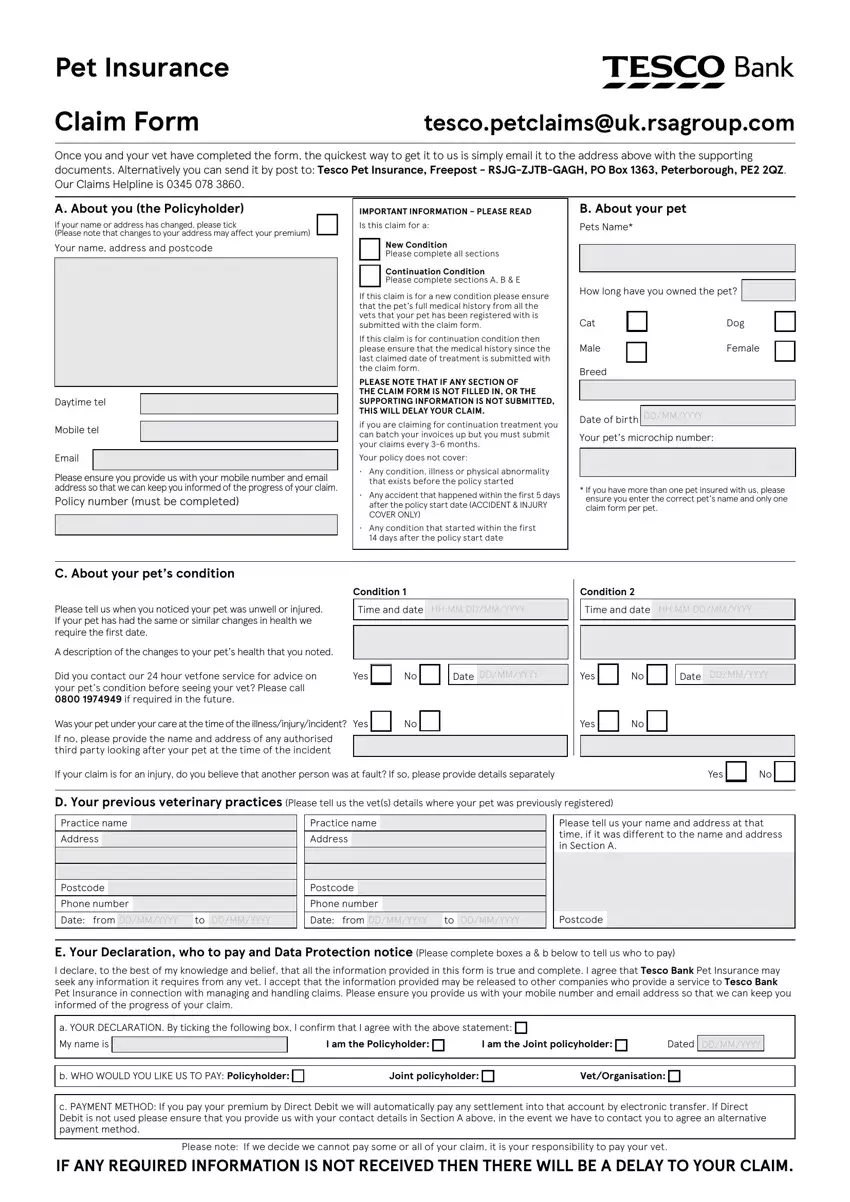
Write the information in Please tell us when you noticed, A description of the changes to, Did you contact our hour vetfone, Time and date, Time and date, Yes, Date, Yes, Date, Was your pet under your care at, Yes, If your claim is for an injury do, Yes, D Your previous veterinary, and Practice name.
It's essential to identify the important information from the b WHO WOULD YOU LIKE US TO PAY, Joint policyholder, VetOrganisation, c PAYMENT METHOD If you pay your, and Please note If we decide we cannot part.

The space F The vet must fill in this, Please advise when the pet was, If this pet was referred to you, If a house call was made you must, Postcode, Please advise if you are a member, Yes, If any part of this claim is for, Date, Treatment recommended Yes, Treatment was carried out Yes, If the pet was seen out of hours, What is the diagnosis of the, Condition, and Condition should be where one can put both sides' rights and responsibilities.
End up by checking the following areas and preparing them as required: If yes please advise the previous, Yes, Please tell us the date that the, Date, Date of death, From, Yes, Date of death, Date, Has this pet had this condition or, Yes, Yes, If Yes we will need the medical, The body condition score for the, and Scale please add the score in the.
Step 3: Hit the Done button to save your form. Then it is accessible for upload to your electronic device.
Step 4: It's going to be more convenient to have copies of your form. You can rest assured that we are not going to share or see your data.
