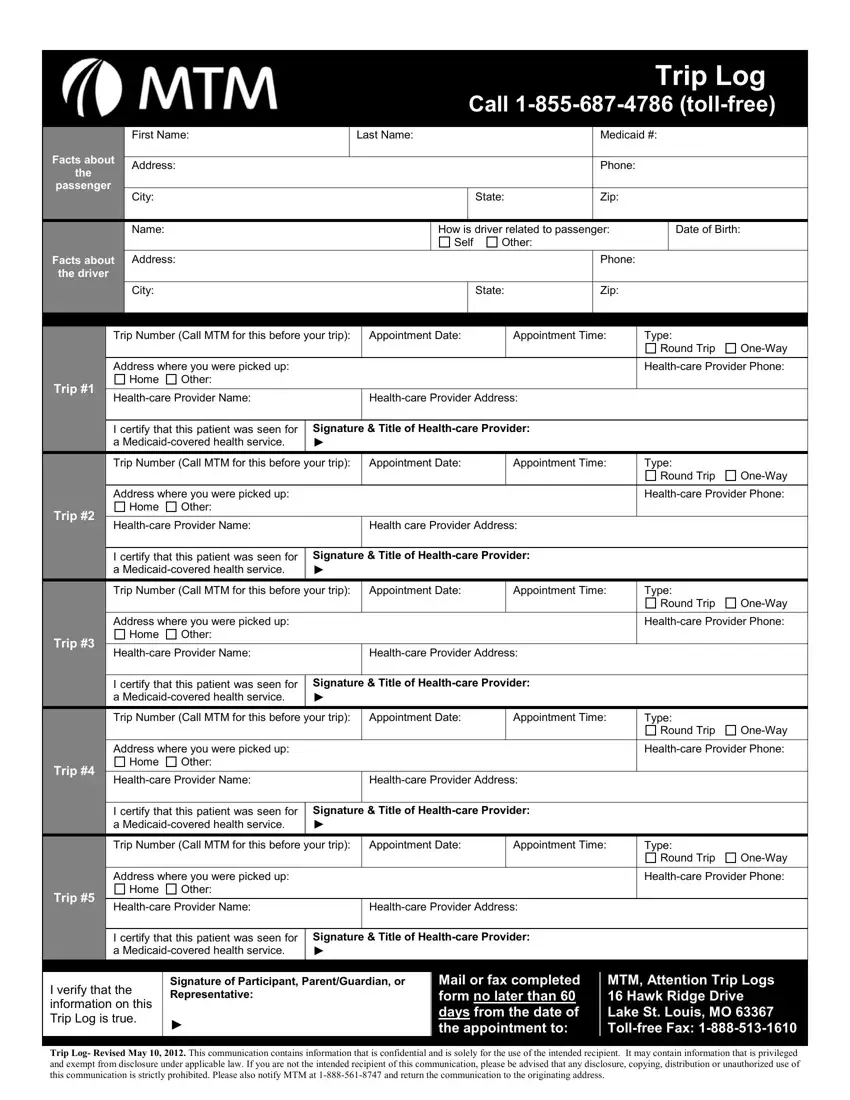
Ensuring that Medicaid recipients can access medical services is vital for their health and well-being. The Trip Log MTM form is a crucial tool in this process, serving as a concrete record of transportation services used by Medicaid beneficiaries to get to and from their healthcare appointments. It requires detailed information about the passenger, such as their name, Medicaid number, and contact details, as well as specifics about their trip(s), including the trip number, appointment date and time, and the type of trip (round trip or one-way). The form also requests information about the driver, how they are related to the passenger, and the healthcare provider's details, including a certification that the patient was seen for a Medicaid-covered health service. Beyond just logging trips, this form acts as a verification tool, ensuring that the transportation provided aligns with Medicaid's goal of facilitating access to necessary healthcare services. It's designed to be submitted within a strict timeframe, requiring the participant, parent, or guardian's signature to affirm the accuracy of the information provided. By meticulously tracking these trips, the form helps maintain the integrity and efficiency of Medicaid's transportation services.
| Question | Answer |
|---|---|
| Form Name | Trip Log Mtm |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | mtm transportation trip log, mtm reimbursement trip log, mtm trip log, trip log form mtm |
