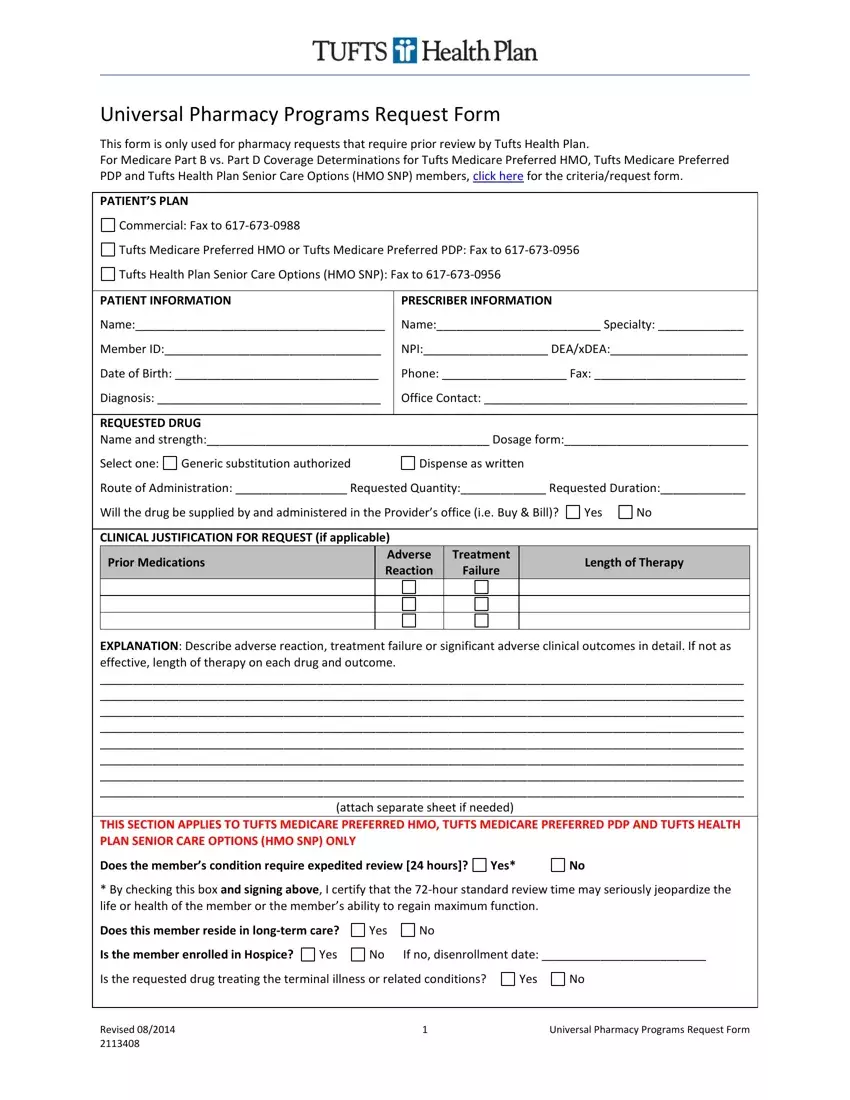
Navigating healthcare processes often involves navigating through detailed forms and requests, especially when it comes to obtaining necessary medications. The Tufts Prior Authorization form plays a crucial role for patients within the Tufts Health Plan, serving as a necessary step for those requiring pharmacy requests that mandate a review before approval. This form is a universal pathway for various patient plans under Tufts, including Commercial, Tufts Medicare Preferred HMO, Tufts Medicare Preferred PDP, and Tufts Health Plan Senior Care Options (HMO SNP), with specific fax numbers dedicated to each. Details it gathers range from patient information such as name, member ID, and diagnosis to prescriber information like specialty and contact numbers. The form delves deeper into the requested drug's specifications, including its name, strength, and dosage, and it accommodates space for clinical justification for the request, highlighting prior medications, treatment failures, and adverse reactions in detail. Additionally, for select Tufts plans, it explores patient conditions that might necessitate expedited review or special considerations, such as residence in long-term care or hospice enrollment. Prescribers are also prompted to provide detailed explanations if the drug is prescribed for conditions not associated with a terminal illness and to furnish rationale for prior authorization or exception requests, indicating if a tier exception is sought for the prescribed medication. The comprehensive nature of this form ensures that both patient and prescriber viewpoints are thoroughly considered, facilitating a detailed review process by Tufts Health Plan.
| Question | Answer |
|---|---|
| Form Name | Tufts Prior Authorization Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | tufts together prior authorization form, tufts interqual forms 2018, tufts health plan prior authorization form, tufts prior authorization |
