
It is easy to prepare forms applying our PDF editor. Revising the oregon uniform support declaration form form is a breeze for those who stick to the next actions:
Step 1: To start out, hit the orange button "Get Form Now".
Step 2: At this point, you are on the document editing page. You can add text, edit present information, highlight particular words or phrases, insert crosses or checks, add images, sign the document, erase unneeded fields, etc.
If you want to create the oregon uniform support declaration form PDF, enter the information for each of the segments:
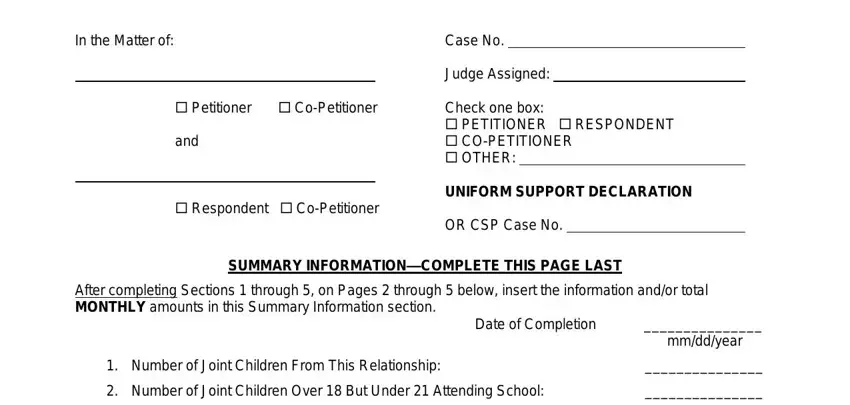
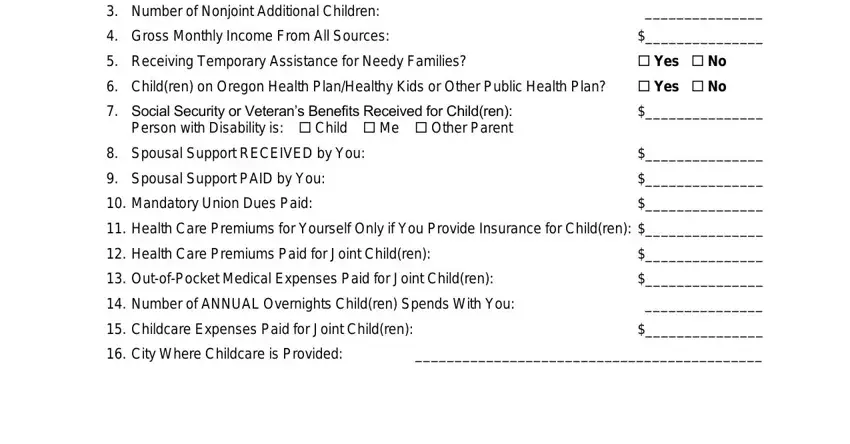
Fill in the Number of Nonjoint Additional, Gross Monthly Income From All, Receiving Temporary Assistance, Yes No, Children on Oregon Health, Yes No, Social Security or Veterans, Spousal Support RECEIVED by You, Spousal Support PAID by You, Mandatory Union Dues Paid, Health Care Premiums for Yourself, Health Care Premiums Paid for, OutofPocket Medical Expenses Paid, Number of ANNUAL Overnights, and Childcare Expenses Paid for Joint areas with any content that is demanded by the program.
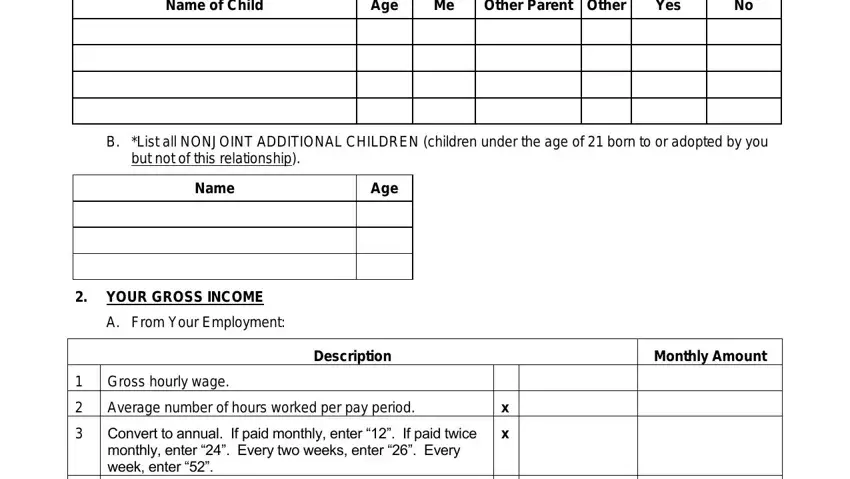
Determine the crucial data in the Name of Child, Age, Other Parent Other, Yes, B List all NONJOINT ADDITIONAL, but not of this relationship, Name, Age, YOUR GROSS INCOME, A From Your Employment, Gross hourly wage, Description, Monthly Amount, Average number of hours worked per, and Convert to annual If paid monthly part.
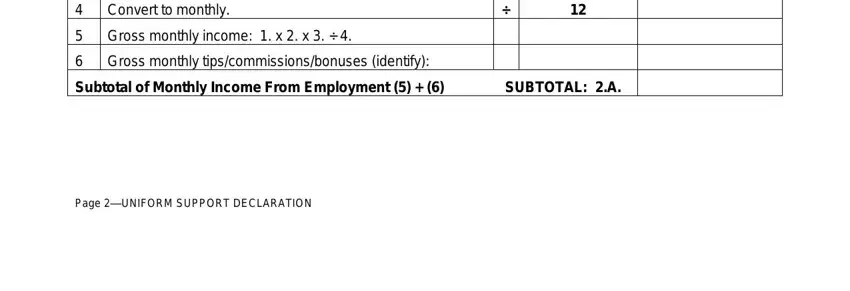
The Convert to monthly, Gross monthly income x x, Gross monthly, Subtotal of Monthly Income From, and Page UNIFORM SUPPORT DECLARATION area will be applied to record the rights or responsibilities of both sides.
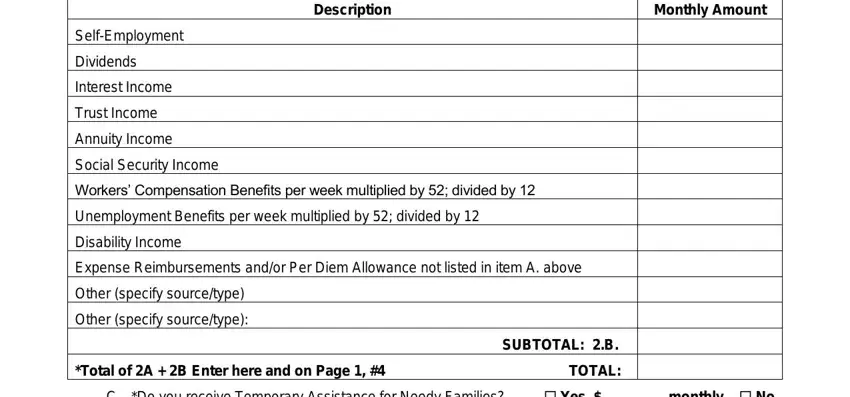
Fill in the document by taking a look at the next fields: Description, Monthly Amount, SelfEmployment, Dividends, Interest Income, Trust Income, Annuity Income, Social Security Income, Workers Compensation Benefits per, Unemployment Benefits per week, Disability Income, Expense Reimbursements andor Per, Other specify sourcetype, Other specify sourcetype, and Total of A B Enter here and on.
Step 3: As soon as you press the Done button, your ready file can be transferred to all of your devices or to email stated by you.
Step 4: Create copies of your form - it will help you refrain from upcoming problems. And don't be concerned - we don't reveal or view your data.
