
 Department of Veterans Affairs
Department of Veterans Affairs 
This PDF editor was made to be as easy as it can be. As you comply with the following actions, the procedure for managing the meds by mail champva file is going to be effortless.
Step 1: Initially, click the orange button "Get Form Now".
Step 2: You can now manage your meds by mail champva. Our multifunctional toolbar permits you to include, erase, adapt, and highlight content or perhaps perform several other commands.
These particular sections will constitute the PDF template that you'll be filling out:
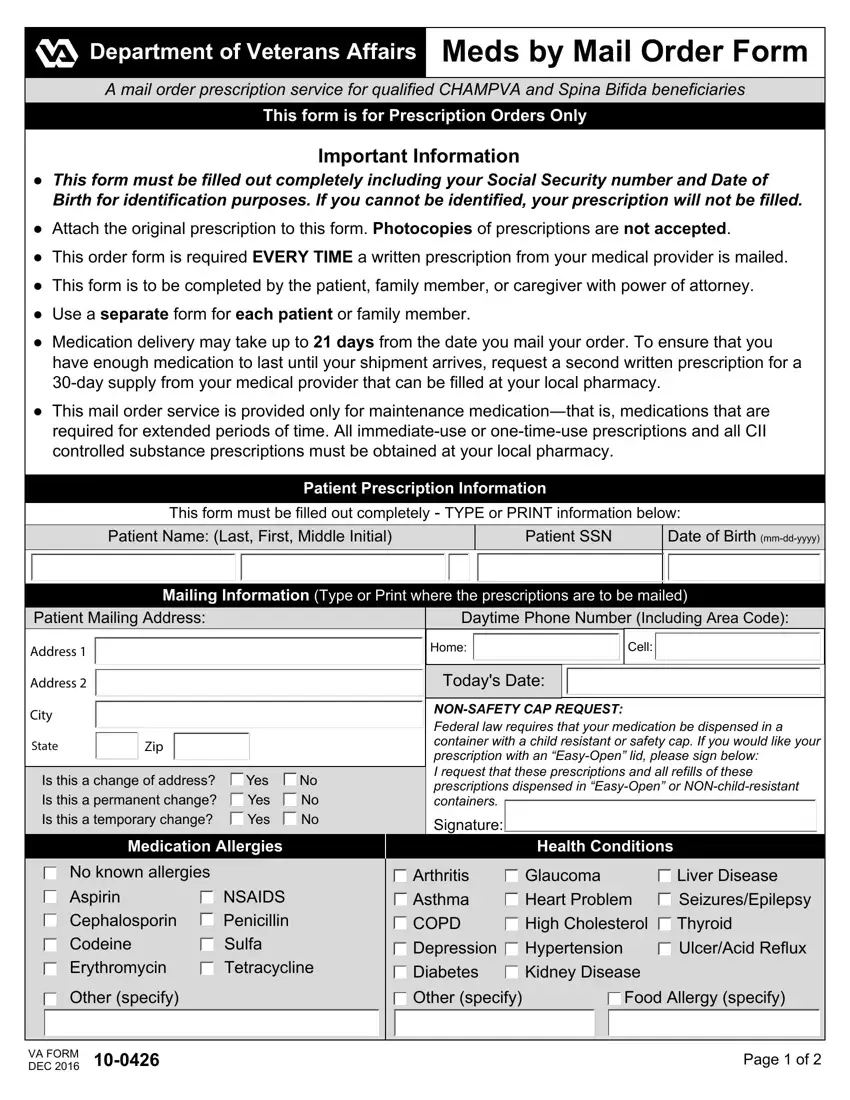
Make sure you enter your details within the segment Patient Name Last First Middle, Patient SSN, Date of Birth mmddyyyy, Patient Mailing Address, Daytime Phone Number Including, Mailing Information Type or Print, Address, Address, City, State, Zip, Is this a change of address Yes No, Medication Allergies, No known allergies, and Aspirin NSAIDS Cephalosporin.
Write the main particulars in Aspirin NSAIDS Cephalosporin, Tetracycline, Other specify, VA FORM JAN, VA FORM DEC, Arthritis Glaucoma Liver Disease, Other specify Food Allergy specify, Page of, and Page of field.

Take the time to specify the rights and responsibilities of the parties within the Provider Information, Provider Name, Provider Contact, VA FORM DEC, and Page of paragraph.
Step 3: Choose the "Done" button. Next, you may export the PDF file - download it to your electronic device or send it through electronic mail.
Step 4: To avoid possible future troubles, you need to get a minimum of a few copies of every document.
