You can easily create the Va Form 10 3542 form with our PDF editor. The following steps will help you quickly create your document.
Step 1: Press the "Get Form Now" button to start out.
Step 2: You are now allowed to change Va Form 10 3542. You have lots of options with our multifunctional toolbar - you can include, eliminate, or alter the text, highlight its certain elements, and conduct similar commands.
These segments will compose the PDF template that you'll be creating:

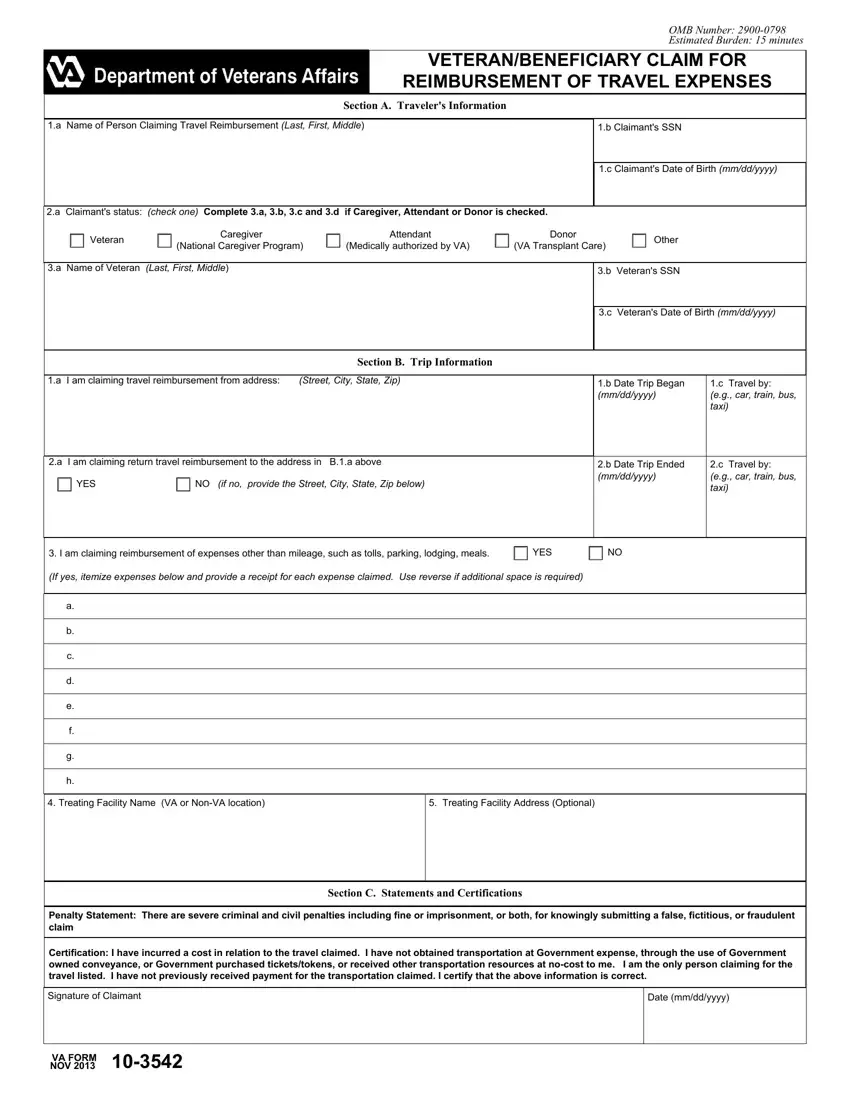
Type in the expected details in the Treating Facility Name VA or, Treating Facility Address Optional, Section C Statements and, Penalty Statement There are severe, and Certification I have incurred a field.

The program will request you to provide certain important details to instantly fill out the part Signature of Claimant, Date mmddyyyy, and VA FORM NOV.

The Question ac, The form may be presented in, Addresses of VA health care, Application for travel, beyond days may occur when claim, Receipts are required for, ferry fares meals lodging and, Application will be evaluated to, Payment will be by electronic, The Paperwork Reduction Act of, and Privacy Act Information VA is section is the place where each party can place their rights and obligations.

Step 3: Press the Done button to confirm that your finished form can be exported to any type of gadget you end up picking or forwarded to an email you specify.
Step 4: Be sure to stay clear of potential issues by making minimally two duplicates of the document.
