It really is not hard to prepare the united healthcare vision claim form. Our editor was created to be enable you to fill in any document swiftly. These are the four steps to take:
Step 1: Hit the "Get Form Now" button to get started on.
Step 2: The file editing page is now open. Include text or update present details.
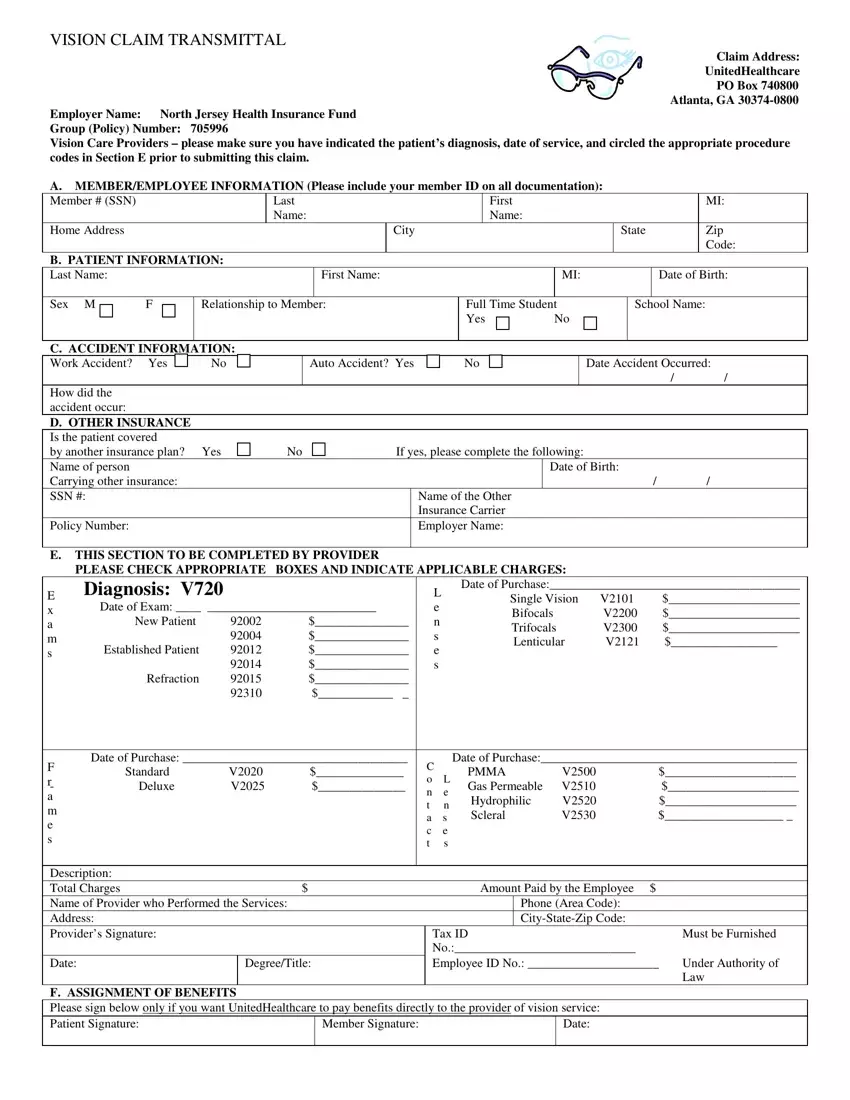
The PDF template you plan to fill out will consist of the next sections:
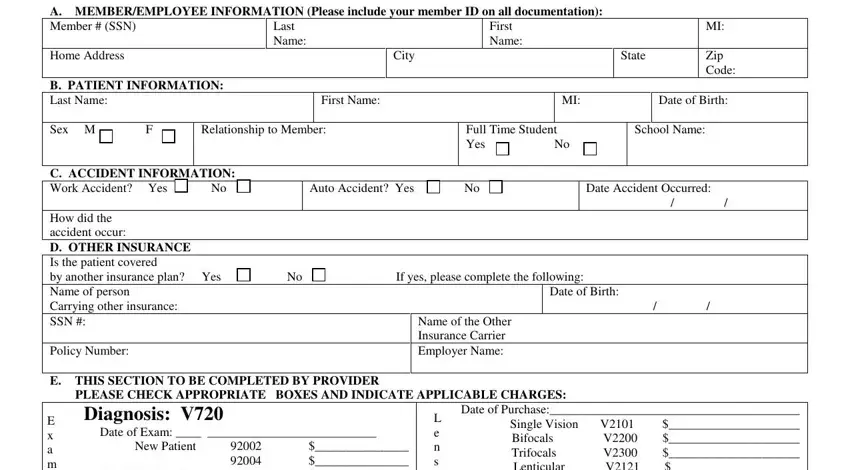
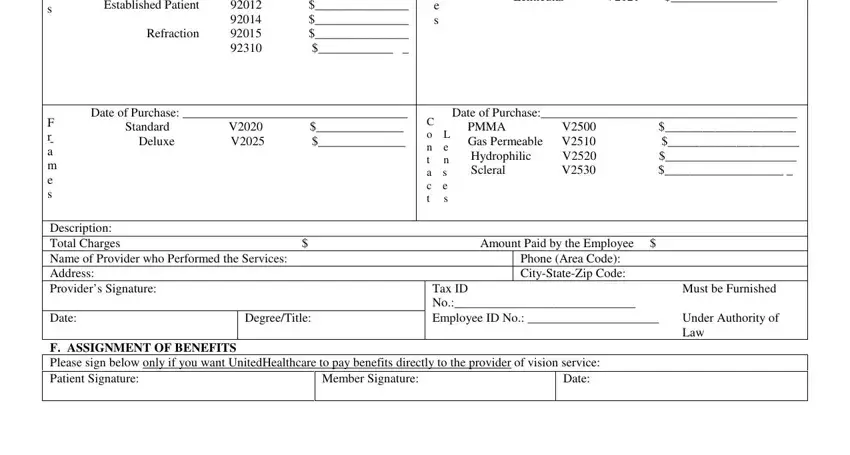
You have to enter the crucial information in the E THIS SECTION TO BE COMPLETED BY, Date of Purchase L Single Vision V, Lenticular V, Date of Purchase F Standard V r, Date of Purchase C PMMA V o L Gas, Description Total Charges Amount, Phone Area Code CityStateZip Code, Date, DegreeTitle, F ASSIGNMENT OF BENEFITS Please, Member Signature, Date, Tax ID No Employee ID No, Must be Furnished, and Under Authority of Law area.
Step 3: Press "Done". You can now export your PDF document.
Step 4: To prevent yourself from possible upcoming complications, please be sure to have as much as a pair of copies of each and every file.
