
 N/A
N/A 
 No
No 
 Yes: Date Certified: __________ Cert. #: ____________
Yes: Date Certified: __________ Cert. #: ____________
 N/A
N/A 
 No
No 
 Yes: Date you met the qualifications: ______________
Yes: Date you met the qualifications: ______________

 Yes
Yes 
 No
No
 Yes
Yes 
 No
No 
 Yes
Yes 
 No
No
 Yes
Yes 
 No
NoIt's super easy to prepare the bbs experience verification. Our PDF editor was created to be assist you to prepare any form efficiently. These are the steps to follow:
Step 1: On this web page, hit the orange "Get form now" button.
Step 2: It's now possible to modify your bbs experience verification. This multifunctional toolbar will allow you to add, erase, adapt, and highlight content as well as carry out other sorts of commands.
Create the following parts to create the template:
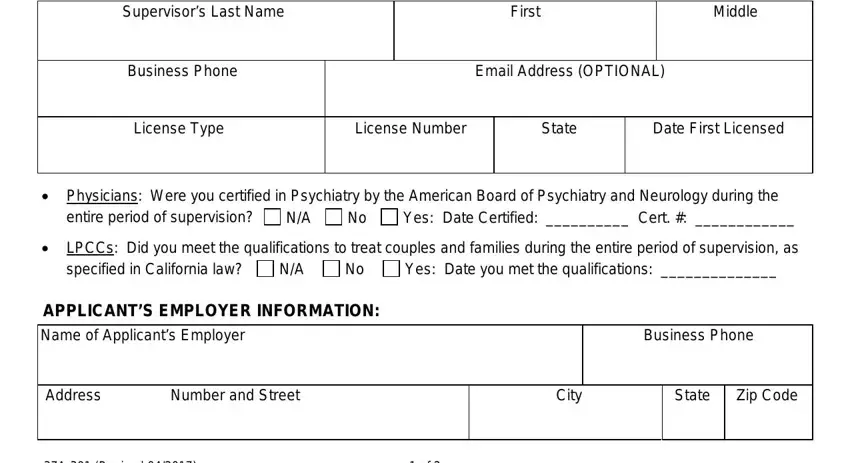
Fill in the Supervisors Last Name, First, Middle, Business Phone, Email Address OPTIONAL, License Type, License Number, State, Date First Licensed, Physicians Were you certified in, entire period of supervision, D D No, Yes Date Certified Cert, LPCCs Did you meet the, and specified in California law fields with any information that is required by the system.
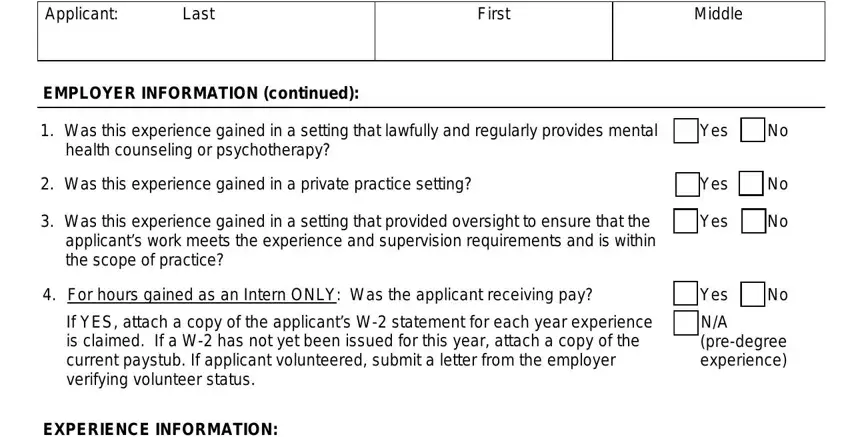
You will be required to enter the details to let the software prepare the box Applicant, Last, First, Middle, EMPLOYER INFORMATION continued, Was this experience gained in a, Yes, health counseling or psychotherapy, Was this experience gained in a, Was this experience gained in a, For hours gained as an Intern, If YES attach a copy of the, Yes, Yes, and D D.
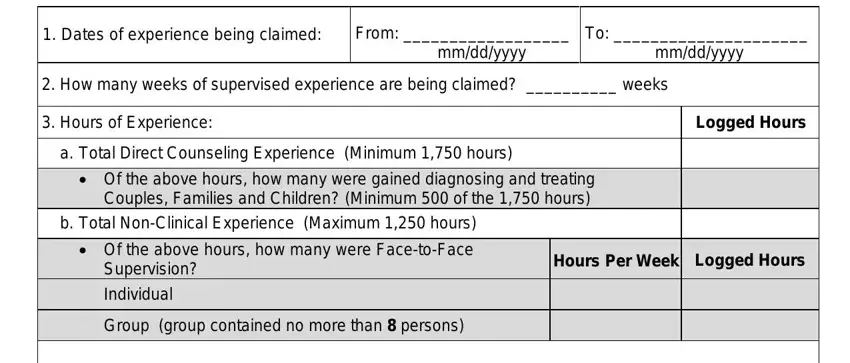
For field EXPERIENCE INFORMATION, Dates of experience being claimed, From, mmddyyyy, To mmddyyyy, How many weeks of supervised, Hours of Experience, Logged Hours, a Total Direct Counseling, Of the above hours how many were, b Total NonClinical Experience, Supervision, Individual, Group group contained no more than, and Hours Per Week Logged Hours, indicate the rights and obligations.
Finalize by reading these sections and filling them out correspondingly: NOTE Knowingly providing false, Signature of Supervisor, Date, and A Revised.
Step 3: Click the "Done" button. Now it's possible to export your PDF document to your electronic device. As well as that, it is possible to deliver it via electronic mail.
Step 4: It is better to create copies of the file. You can rest assured that we won't distribute or view your particulars.
