
The 4501 DHSR HCPR form can be completed online in no time. Simply use FormsPal's PDF tool to get the job done in a timely fashion. This tool is constantly developing to grant the best user experience possible. For other North Carolina health forms, you can also explore the DHSR AC 4207 and the health care professional form. All it requires is a few basic steps:
Step 1: Simply press the "Get Form Button" above on this webpage to launch our pdf file editing tool. This way, you'll find all that is needed to work with your file.
Step 2: With this advanced PDF editing tool, you're able to accomplish more than merely complete blanks. Express yourself and make your docs seem professional with custom text added in, or optimize the original input to perfection. You can also incorporate any images and sign the PDF off.
Be mindful while filling in this form. Make certain each and every field is done correctly.
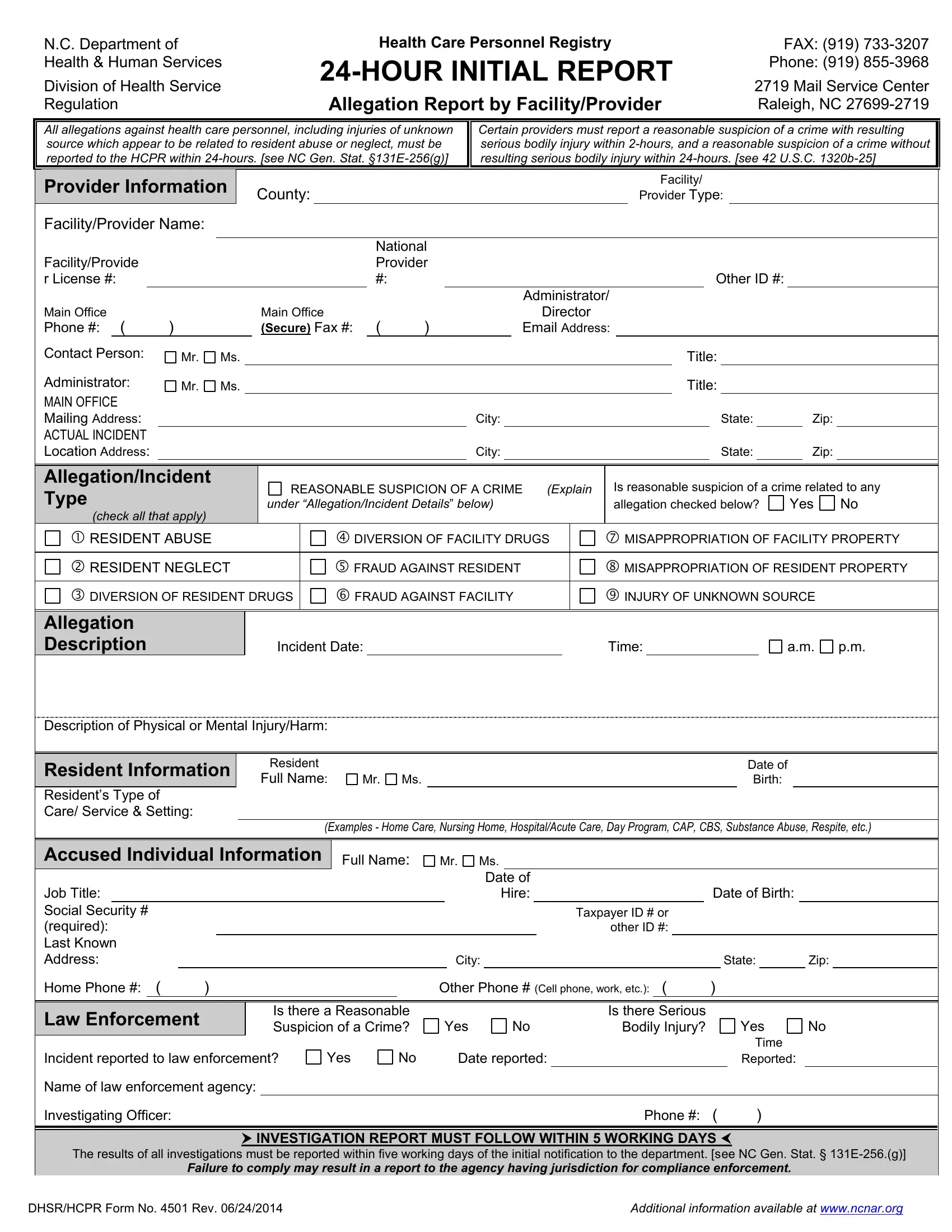
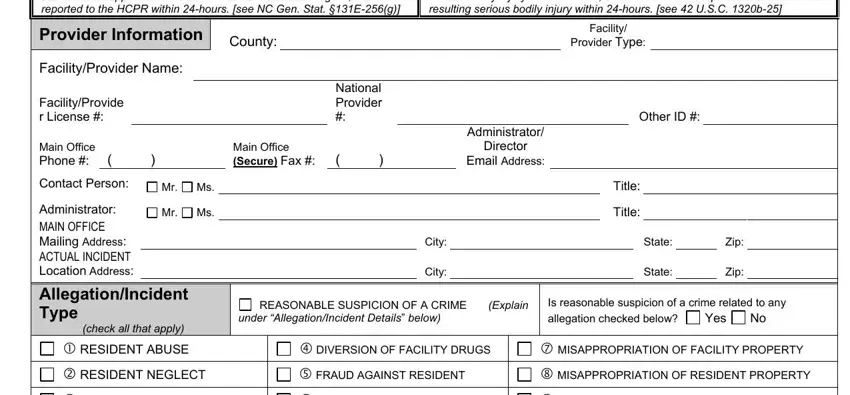
1. The 4501 DHSR HCPR form necessitates specific information to be typed in. Make certain the following fields are finalized:
2. Once this part is filled out, proceed to type in the relevant information in all these: DIVERSION OF RESIDENT DRUGS, FRAUD AGAINST FACILITY, INJURY OF UNKNOWN SOURCE, Allegation Description, Incident Date, Time, Description of Physical or Mental, Resident Information Residents, Resident, Full Name, Date of Birth, Examples Home Care Nursing Home, Accused Individual Information, Job Title Social Security, and Home Phone.
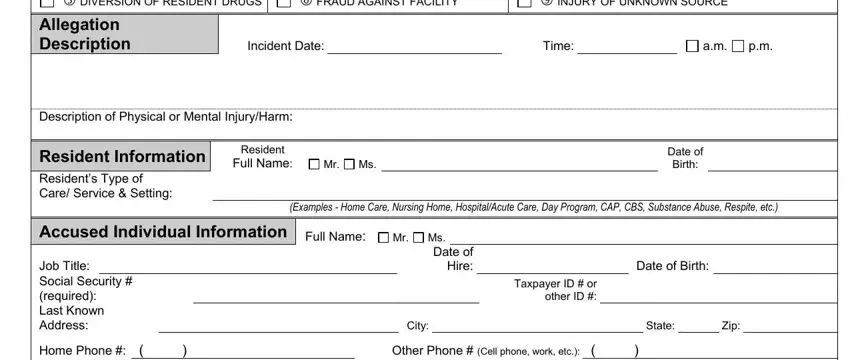
Always be really attentive while completing Full Name and Incident Date, since this is where most users make some mistakes.
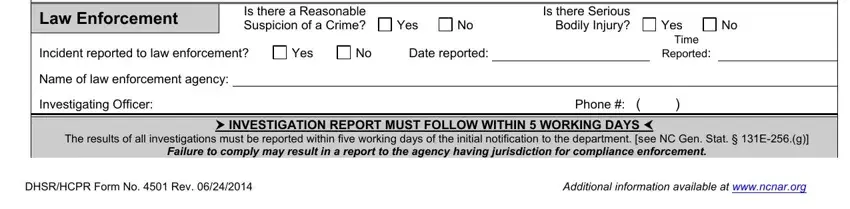
3. In this specific stage, check out Law Enforcement, Is there a Reasonable Suspicion of, Yes, Is there Serious Bodily Injury, Incident reported to law, Yes, Date reported, Name of law enforcement agency, Investigating Officer, Yes, Time, Reported, Phone, The results of all investigations, and INVESTIGATION REPORT MUST FOLLOW. All these have to be completed with greatest precision.
4. To go ahead, the next stage requires filling out a few form blanks. These include Print Name and Title of Person, and Signature of Person Preparing, which are fundamental to continuing with this particular document.
5. To wrap up your form, the particular area has a couple of extra blank fields. Entering DHSR HCPR Form No Rev, and Additional information available will certainly wrap up the process and you're going to be done in no time!

Step 3: Once you have looked once again at the information in the blanks, simply click "Done" to complete your document creation. Create a free trial subscription with us and obtain direct access to the 4501 DHSR HCPR form, downloadable, emailable, and editable in your FormsPal cabinet. With FormsPal, you can easily complete documents without worrying about database incidents or records getting distributed. Our secure platform makes sure that your personal details are maintained safely.