Editing this First Report of Injury in our online PDF editor is simple and takes only a few minutes. Follow these four steps to fill out, sign, and download your completed form:
Step 1: Click the "Get form here" button to open the document in the editor.
Step 2: Start editing the form. The toolbar lets you insert text, checkboxes, dates, and signatures in any field.
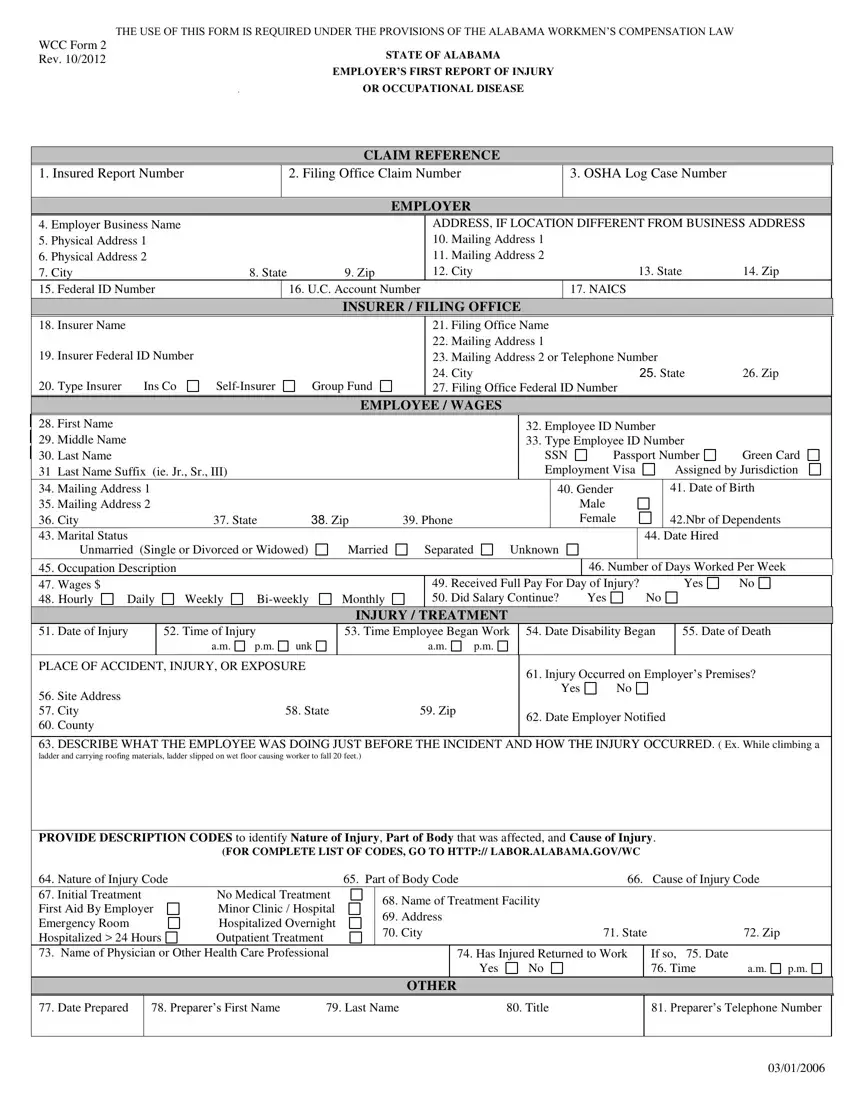
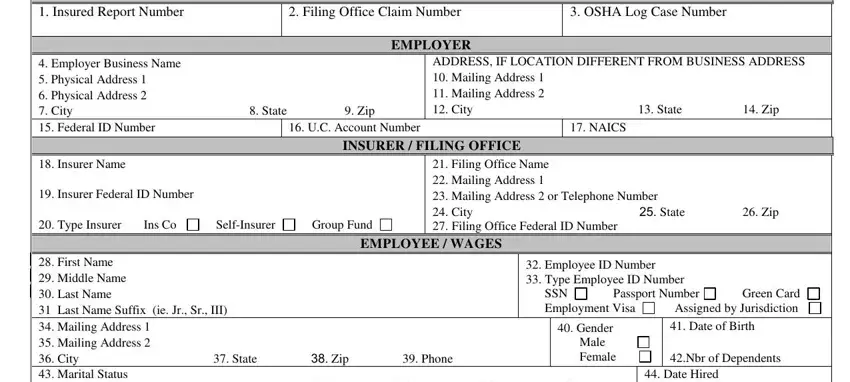
Fill in the employee name, injury date, injury time, date disability began, number of days worked per week, wage type (weekly, biweekly, monthly, daily, or unknown), and marital status (married or separated).
Next, complete the Nature of Injury Code, Part of Body Affected, Name of Treatment Facility, Return to Work status (Yes or No), Return Date, Date Prepared, Preparer Name, and Preparer Phone Number.
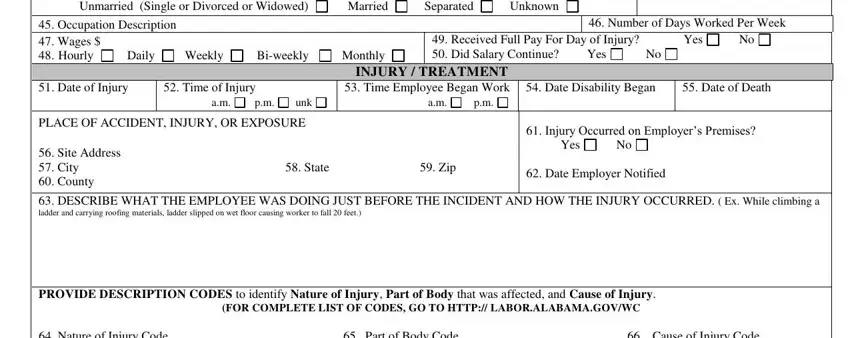
Verify the employer information, insurer details, and incident description in the remaining sections of the form.
Step 3: Click Done to save your completed form. Download a copy to your device.
Step 4: Save a duplicate for your records. Your data is kept private and is never shared.
After You Submit the Form
Send the completed form to your insurer and to the Alabama Workers' Compensation Division within the 15-day deadline. Your insurer will open a claim file and contact the injured employee. Keep a timestamped copy for your own records in case of any dispute.
Frequently Asked Questions
What is the Alabama First Report form used for?
Employers use this document to notify the Alabama Workers' Compensation Division and their insurer of a workplace injury or occupational disease. It opens the workers' compensation claim and creates an official incident record. Failure to file may result in fines and loss of certain insurer protections.
Is the form required for all injuries?
Yes. Alabama law requires filing whenever an employee misses work due to a job-related injury or illness. File the form even if the injury appears minor at first, since symptoms can worsen over time and claim rights depend on timely reporting.
Where should I send the completed form?
Submit to the Alabama Workers' Compensation Division and send a copy to your insurance carrier. Your insurer handles the claim review and benefit determination for the injured worker.
Related Workers' Compensation Forms
After filing, you may also need these related workplace injury documents:
- Workers' Compensation Injury Report – general workplace injury documentation
- First Injury Report – standard first injury report template
- Workers' Compensation C-4 Form – for continued treatment documentation
- Alabama Incident Report – for incidents not immediately resulting in injury
- Workers' Compensation Intake Form – for collecting employee injury information
