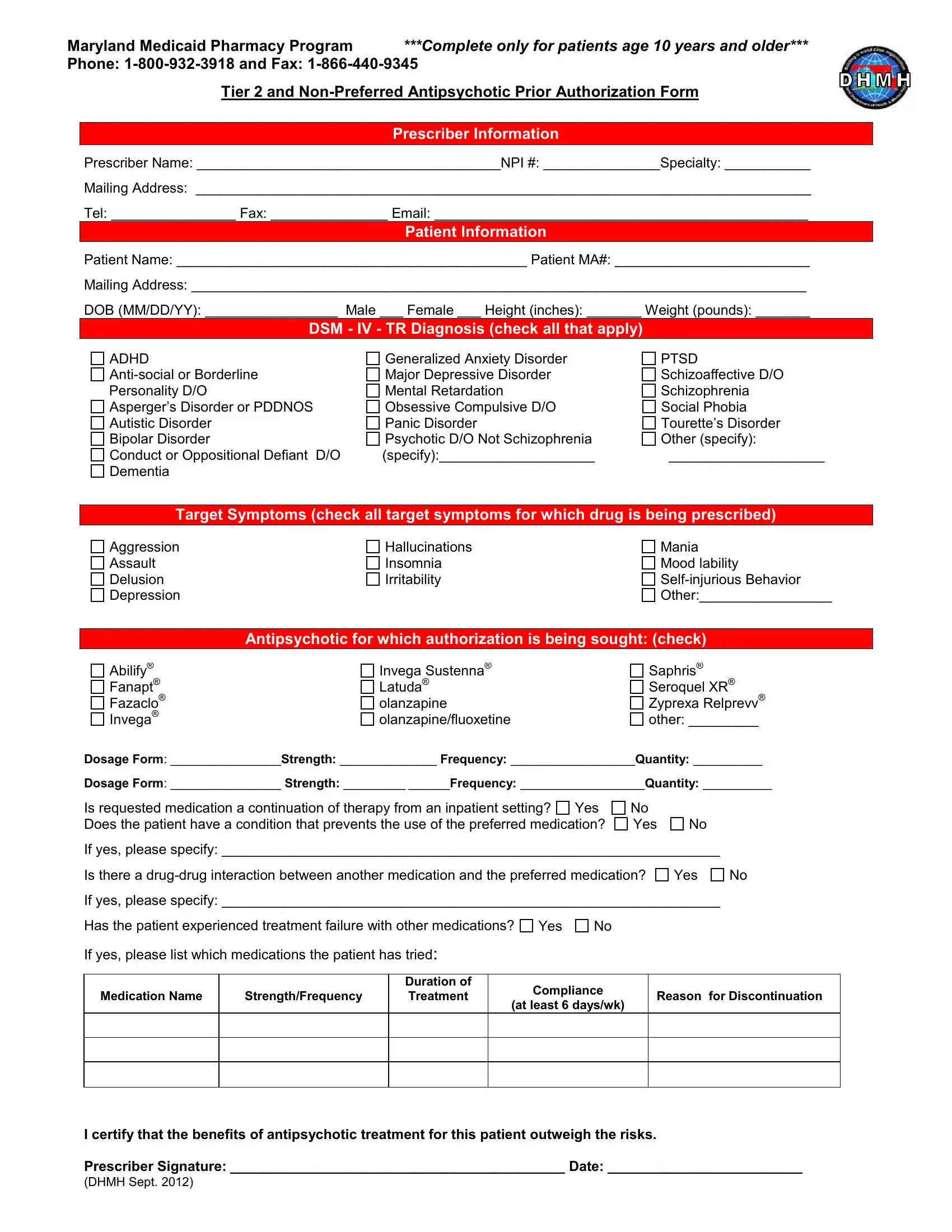
In the realm of Maryland's Medicaid Pharmacy Program, the Antipsychotic Prior Authorization form emerges as a crucial document, specifically designed for the oversight of antipsychotic medication prescriptions for patients aged 10 years and older. At its core, this form serves as an essential tool to ensure that patients receive the most appropriate medications for their conditions, under the scrutiny of Medicaid's regulations. By requiring detailed prescriber information, including name, specialty, contact details, and National Provider Identifier (NPI), along with comprehensive patient data such as demographics, diagnosis, and target symptoms, the form facilitates a meticulous review process. It covers a spectrum of DSM - IV - TR diagnoses and specifies the antipsychotic medication requested, dosage, and frequency, addressing whether the request is for a continuation of therapy from an inpatient setting or if there are specific reasons preventing the use of preferred medication. Moreover, the form probes into possible drug-drug interactions and past treatment failures, ensuring that the prescribed antipsychotics are not only necessary but also the safest and most effective choice for the patient. This validation is underscored by the prescriber's certification that the benefits of the treatment outweigh the associated risks, underscored by their signature and the date, thereby highlighting the form’s role in upholding the judicious use of antipsychotic medications within the parameters of Maryland Medicaid's Pharmacy Program.
| Question | Answer |
|---|---|
| Form Name | Antipsychotic Prior Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | how to fill out medical prior authorization university of maryland, md antipsychotic form, maryland physician care prior auth form, maryland medicaid prior authorization form antipsychotic |
Maryland Medicaid Pharmacy Program ***Complete only for patients age 10 years and older*** Phone:
Tier 2 and
Prescriber Information
Prescriber Name: _______________________________________NPI #: _______________Specialty: ___________
Mailing Address: _______________________________________________________________________________
Tel: ________________ Fax: _______________ Email: ________________________________________________
Patient Information
Patient Name: _____________________________________________ Patient MA#: _________________________
Mailing Address: _______________________________________________________________________________
DOB (MM/DD/YY): _________________ Male ___ Female ___ Height (inches): _______ Weight (pounds): _______
DSM - IV - TR Diagnosis (check all that apply)
ADHD
Asperger’s Disorder or PDDNOS Autistic Disorder
Bipolar Disorder
Conduct or Oppositional Defiant D/O Dementia
Generalized Anxiety Disorder Major Depressive Disorder Mental Retardation Obsessive Compulsive D/O Panic Disorder
Psychotic D/O Not Schizophrenia (specify):____________________
PTSD
Schizoaffective D/O
Schizophrenia
Social Phobia
Tourette’s Disorder
Other (specify):
____________________
Target Symptoms (check all target symptoms for which drug is being prescribed)
Aggression
Assault
Delusion
Depression
Hallucinations |
Mania |
Insomnia |
Mood lability |
Irritability |
|
|
Other:_________________ |
Antipsychotic for which authorization is being sought: (check)
Abilify®
Fanapt®
Fazaclo®
Invega®
Invega Sustenna® Latuda® olanzapine olanzapine/fluoxetine
Saphris® Seroquel XR® Zyprexa Relprevv® other: _________
Dosage Form: ________________Strength: ______________ Frequency: __________________Quantity: __________
Dosage Form: ________________ Strength: _________ ______Frequency: __________________Quantity: __________
Is requested medication a continuation of therapy from an inpatient setting? |
Yes |
No |
Does the patient have a condition that prevents the use of the preferred medication? |
Yes |
|
No
If yes, please specify: ________________________________________________________________
Is there a
If yes, please specify: ________________________________________________________________
Has the patient experienced treatment failure with other medications? Yes No
No
If yes, please list which medications the patient has tried:
Medication Name
Strength/Frequency
Duration of Treatment
Compliance
(at least 6 days/wk)
Reason for Discontinuation
I certify that the benefits of antipsychotic treatment for this patient outweigh the risks.
Prescriber Signature: ___________________________________________ Date: _________________________
(DHMH Sept. 2012)