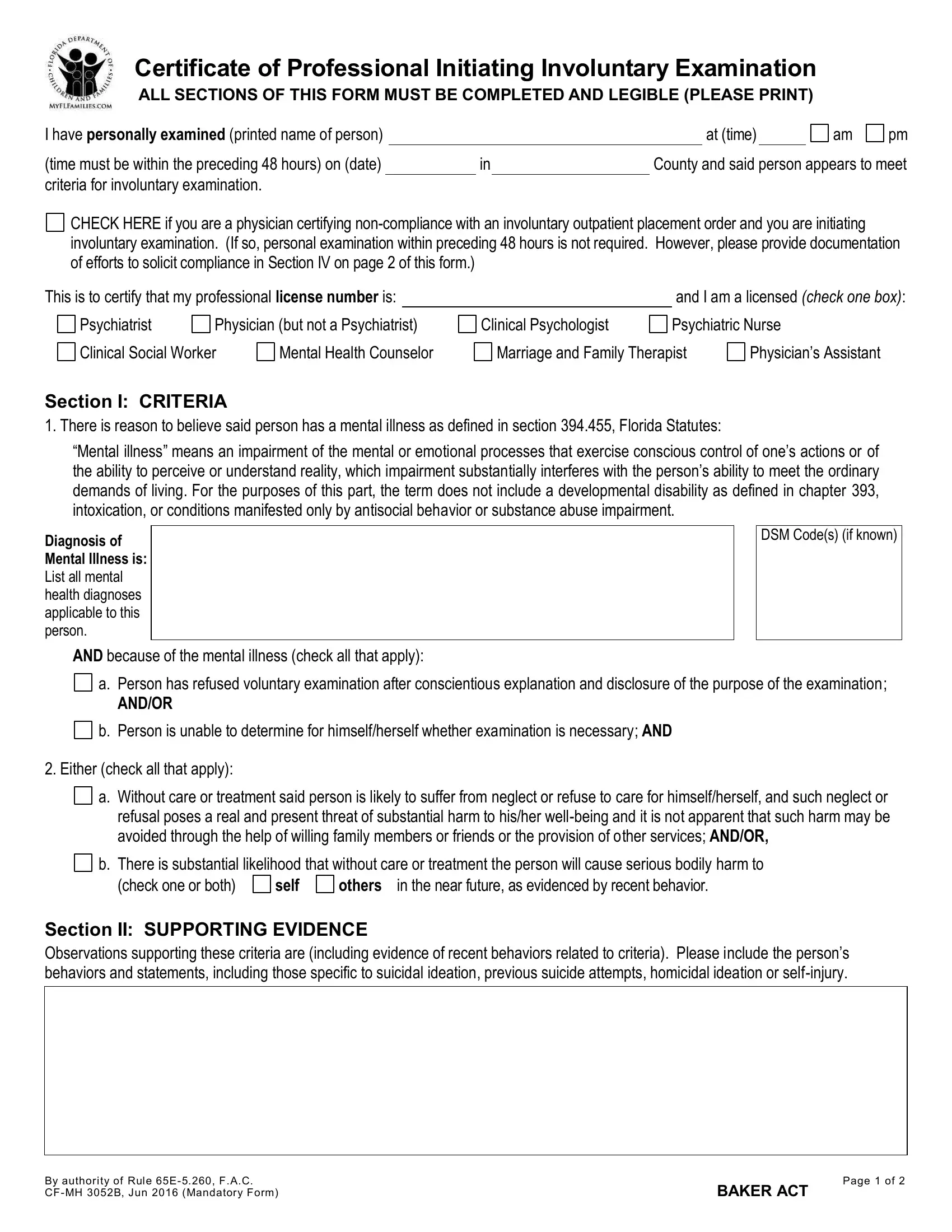
The Baker Act form serves as a critical instrument within the legal and health care landscape, particularly in the state of Florida, for initiating an involuntary examination of an individual who is believed to have a mental illness that could result in harm to themselves or others. The form, officially titled "Certificate of Professional Initiating Involuntary Examination," requires meticulous completion by licensed professionals, including psychiatrists, physicians, clinical social workers, mental health counselors, clinical psychologists, psychiatric nurses, marriage and family therapists, or physician’s assistants. These professionals must have personally examined the individual within the preceding 48 hours (with specific exceptions for non-compliance with an involuntary outpatient placement order) and determined that the individual meets the criteria for involuntary examination due to their mental state. The form outlines specific diagnostic criteria and supports the examination with detailed observations of the person's behavior and statements, references to mental health diagnoses adhering to the DSM codes, and the potential risks of neglect or harm without treatment. Additionally, it includes provisions for cases of non-compliance with involuntary outpatient placement orders, requiring documentation of efforts to encourage compliance. Information that aids law enforcement in locating the individual for examination is also a critical component of the form, ensuring that all necessary details for identifying and safely transporting the person are available. In essence, the Baker Act form is an essential document that enables licensed professionals to legally initiate steps crucial for the care and safety of individuals displaying significant mental health concerns, thereby playing a vital role in the broader efforts to manage mental health crises effectively.
| Question | Answer |
|---|---|
| Form Name | Baker Act Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | baker act florida form, baker act form florida pdf, florida baker act form pdf, florida baker act form |