
Use the steps below to complete the Wisconsin Care Immunization Form for your child's childcare enrollment. The childcare center requires a completed immunization record within 30 school days of your child's start date.
Step 1: Gather your child's immunization history
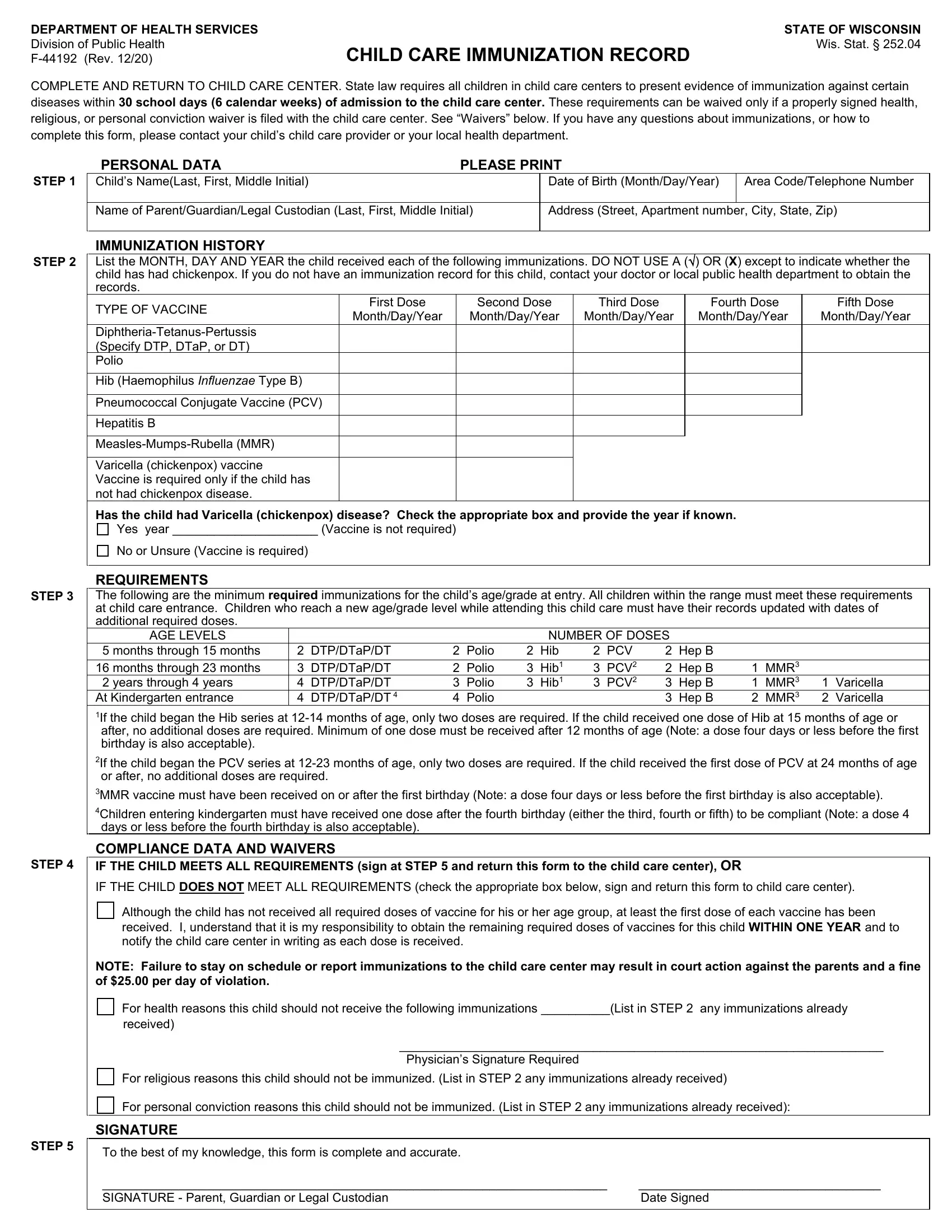
Before filling out the form, collect your child's complete vaccination record from your pediatrician or previous childcare provider. You will need the name of each vaccine and the date each dose was administered. If you do not have a copy of your child's immunization record, contact your child's doctor or check with your state's immunization registry for vaccination records on file.
Step 2: Enter the child's personal information
Write the child's full legal name, date of birth, and the enrollment date at the childcare center. Provide the parent or guardian's name and contact information in the designated fields. This section links the immunization record to the correct child care enrollment file at the center.
Step 3: Document each required vaccine dose
List each required vaccine by name and record the date each dose was administered. The form includes rows for diseases such as diphtheria, tetanus, pertussis, polio, measles, mumps, rubella, varicella, hepatitis B, and Hib. Enter dates in month, day, and year format. Leave a row blank only if the child has not yet received that dose and is not exempt from that requirement.
Step 4: Indicate any applicable exemptions
If your child qualifies for an exemption from one or more required vaccines, check the appropriate exemption category on the form. The Care Immunization Form accepts three exemption types: medical, religious, and personal conviction. A licensed physician must sign the form to support a medical exemption claim. Keep a copy of any supporting documentation your childcare provider may request to process the exemption.
Step 5: Sign and submit the form
The parent or guardian must sign and date the declaration at the bottom to confirm the accuracy of all information provided. Submit the original to the childcare center and keep a copy for your own records. If you need additional documents for enrollment, see the child enrollment packet and the child care incident report used alongside this immunization form.