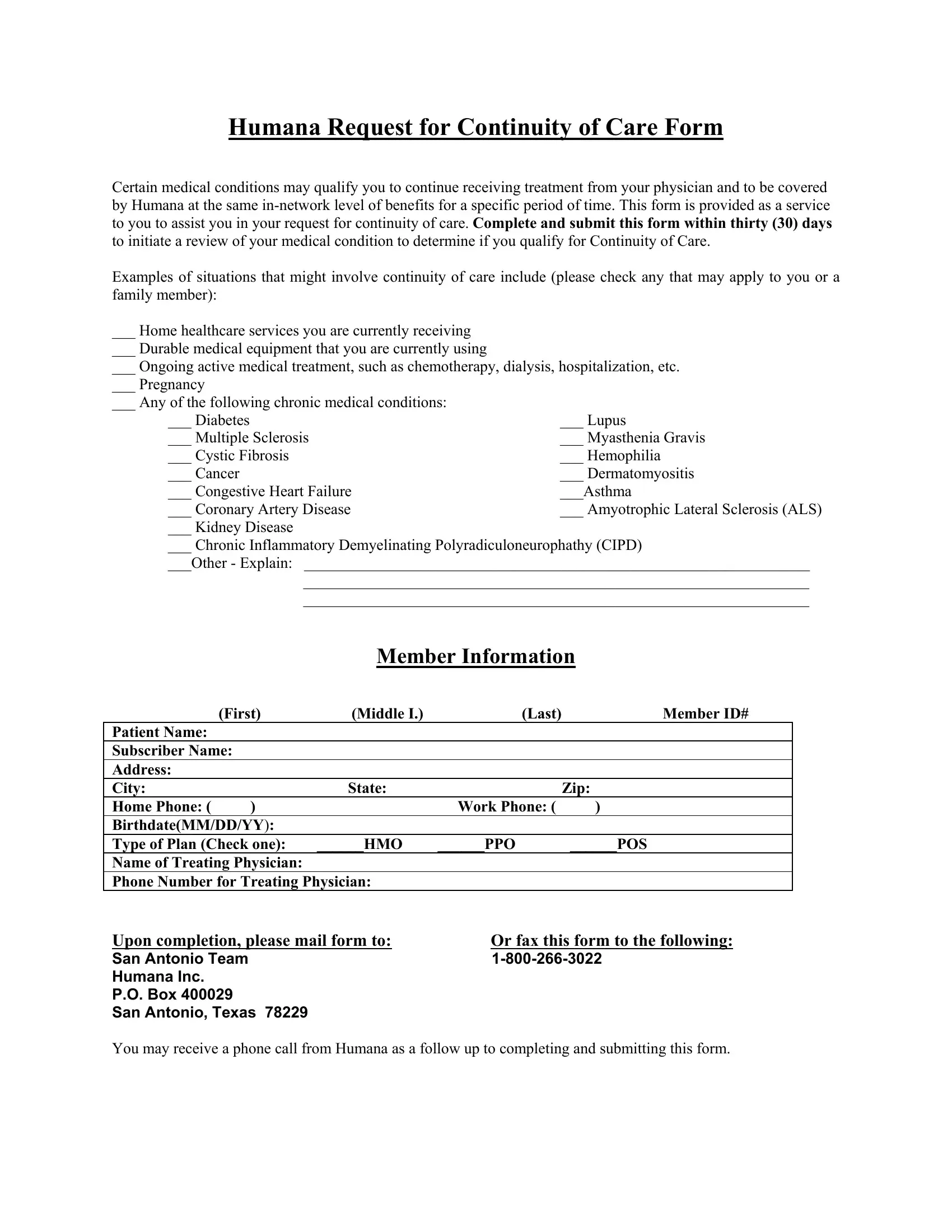
When navigating the complexities of healthcare, especially during transitions in insurance coverage or changes in healthcare providers, understanding how to maintain the continuity of your care is paramount. The Humana Request for Continuity of Care Form serves as a crucial tool for individuals facing such circumstances, ensuring they can continue receiving treatment from their current physicians under the same in-network level of benefits for a designated period. This assistance is invaluable for those requiring uninterrupted access to home healthcare services, durable medical equipment, or ongoing medical treatment for conditions ranging from pregnancy to chronic illnesses like diabetes, cancer, or heart disease. By completing and submitting this form within the required thirty-day window, patients can initiate a review process to determine their eligibility for continued care coverage. This process is not only designed to maintain the health and treatment outcomes of the patient but also to ease the administrative burdens often associated with healthcare transitions. Furthermore, the form includes comprehensive sections for member information and details regarding the treating physician, ensuring a streamlined communication channel with Humana. Submission instructions are clearly outlined, offering options to mail or fax the form, followed by a potential follow-up call from Humana, adding a personal touch to the process.
| Question | Answer |
|---|---|
| Form Name | Humana Continuity Care Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 32 |
| Avg. time to fill out | 6 min 39 sec |
| Other names | humana continuation of care form, humana request of continuety form, humana durable medical equipment forms, humana request for continuity of care form |