
FormsPal's online PDF editor makes it simple to complete and download CC Form 2, the Oklahoma Workers' Compensation Employer's First Notice of Injury. Follow the steps below to fill out the form online in minutes.
How to Fill Out Oklahoma CC Form 2 Online
Step 1: Open the CC Form 2 in the FormsPal editor by clicking the "Get Form" button at the top of this page. The form loads instantly without any downloads or software installation.
Step 2: Review and complete all required fields in the editor. You can fill in blank fields, add text, apply your signature, and make other changes to the document before saving.
Completing the Required Form Sections
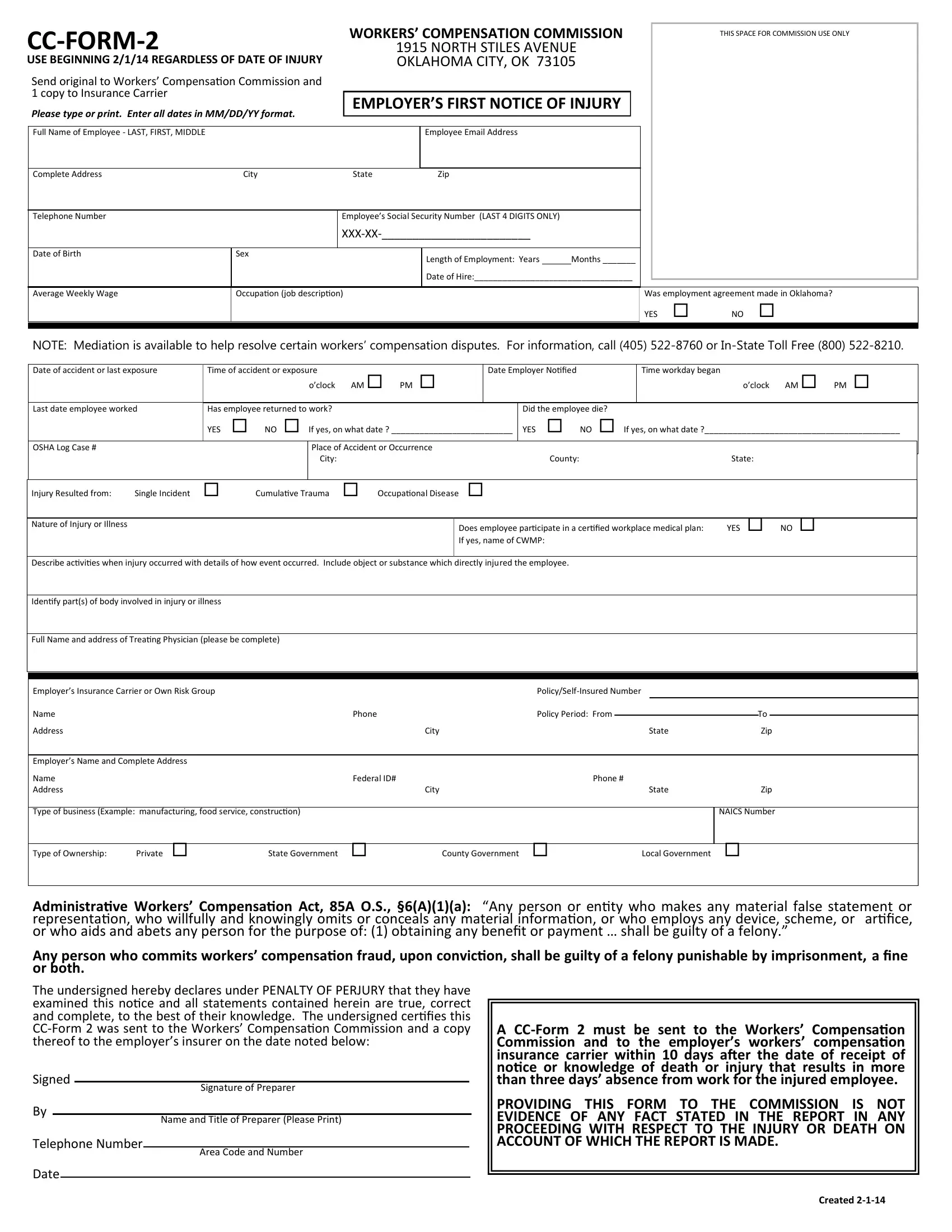
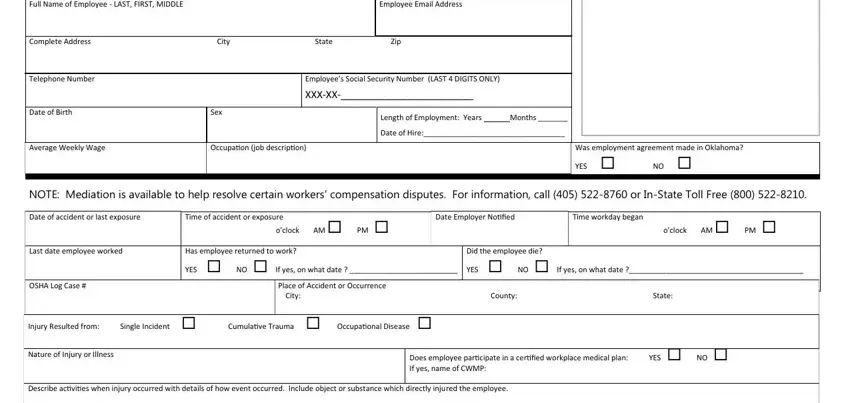
The CC Form 2 contains specific fields about the employee, the employer, and the injury. Fill in each field accurately to avoid delays in the claims process:
1. The first section of the CC Form 2 covers employee identification, employer insurance details, and the type of business. Complete all fields in this section to ensure proper routing to the Workers' Compensation Commission.
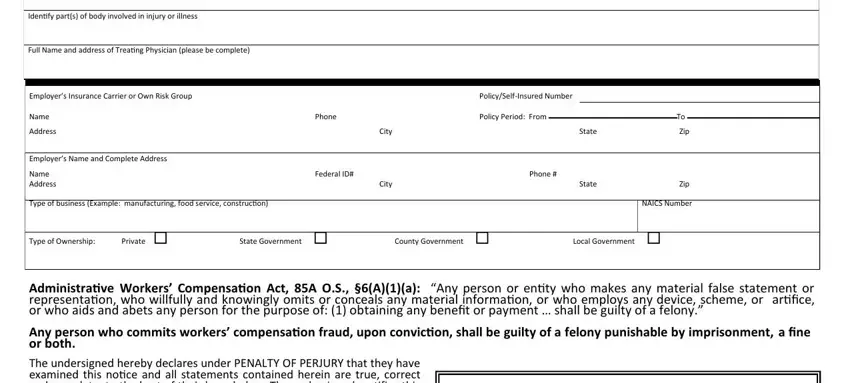
2. The second section includes the employer's identifying information, including name, address, insurance policy number, policy period dates, state, and phone number.
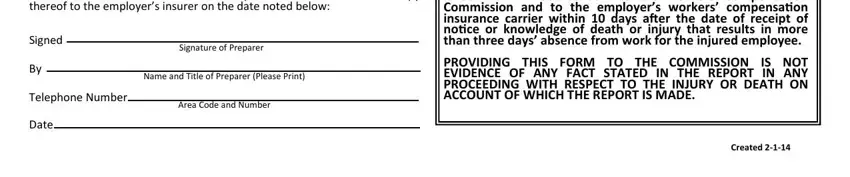
3. The final section requires the preparer's signature, name, title, and telephone number, including area code. Review the Area Code and Number fields carefully. This is the most common area where errors occur.
Step 3: Once you have reviewed all the information, click "Done" to finalize your CC Form 2. Create a free FormsPal account to download the completed form. All edits are automatically saved so you can return and make changes at any time.
Related Workers' Compensation Forms
You may need to file additional workers' compensation forms as part of the injury reporting process. These forms are available free through FormsPal:
- Workers' Compensation Injury Report for documenting workplace injury details
- Workers' Compensation C-4 Form for physician reporting of work-related injuries
- First Injury Report Form for initial documentation of workplace injuries
- Workers' Compensation Intake Form for processing new claims
Frequently Asked Questions About CC Form 2
What is the CC Form 2 used for?
The CC Form 2 is the Oklahoma Workers' Compensation Employer's First Notice of Injury. Employers must file this form with the WCC and their insurance carrier when an employee suffers a work-related injury or illness.
Who completes the CC Form 2?
The employer or an authorized company representative is responsible for completing and filing the CC Form 2 after being notified of a workplace injury or illness.
When must the CC Form 2 be filed?
Employers must file the CC Form 2 promptly after learning of a work-related injury. Timely reporting is required under Oklahoma workers' compensation law to protect the employee's right to benefits.