To complete this form on FormsPal, click the "Fill Out Form" button at the top of the page. The PDF opens in our online editor, where you can type directly into each field, add checkmarks, and save or print when finished. No software download is needed.
Step-by-Step Completion Guide
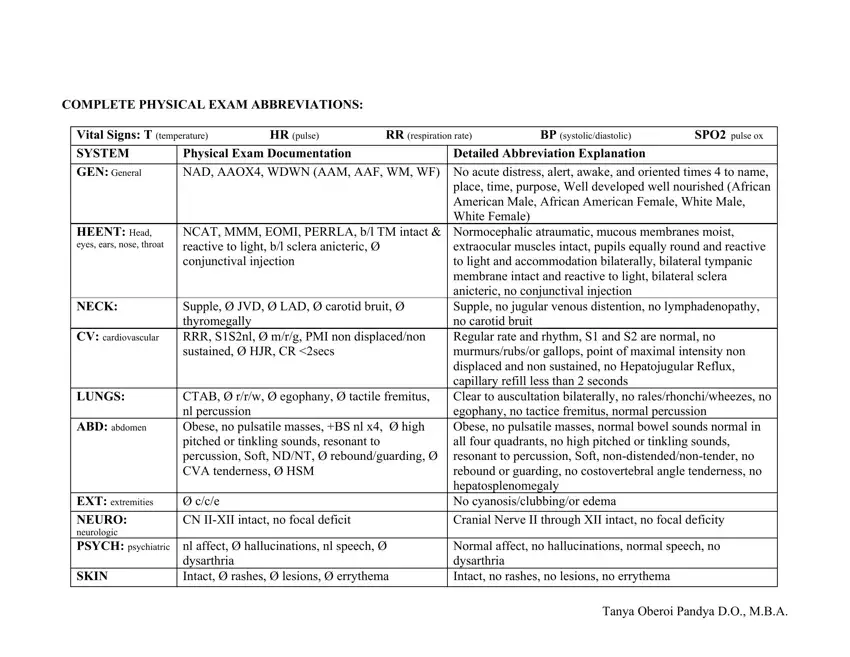
Begin by entering the patient's vital signs at the top of the form. Record temperature, heart rate, respiration rate, blood pressure, and oxygen saturation in the provided fields. Work through each body system section in order, marking normal findings as WNL (within normal limits) and writing specific observations for anything abnormal. Use the abbreviations key printed on the form to complete entries quickly and accurately.
Understanding the Body System Sections
Each row of the form targets one body system. The HEENT section covers the head, eyes, ears, nose, and throat. The CV section records cardiovascular findings such as heart sounds and peripheral pulses. The NEURO section documents reflexes, coordination, and mental status. For each system, write the relevant finding or mark the normal-limit checkbox. Leave a section blank only if the provider did not assess that system during the visit.
Saving and Sharing the Completed Form
After completing all sections, click the download icon to save the PDF to your device. You can also print directly from the editor for a paper copy. If the form requires a provider signature, print it and sign in the designated area before filing it in the patient record or sharing it with the patient.
Related Physical Examination Forms
FormsPal offers several related forms for different clinical and administrative needs. The annual physical examination form is designed for yearly wellness visits. The general physical examination form works for routine checkups and referral documentation. The employee physical form is used for pre-employment and workplace health screenings. The fillable physical exam form provides an alternative format with editable fields for common clinical settings.
