Our PDF editor makes completing this form online straightforward. Follow these steps to fill in and download the document:
Step 1: Click the "Get Form Now" button to begin.
Step 2: You’re now on the document editing page. You may edit, add text, highlight particular words or phrases, put crosses or checks, and insert images.
For every single part, fill out the information asked by the software.
Provide the requested information in the area LIST ANY OTHER SPECIAL MEDICAL OR, A NAME OF MPDPSC REPRESENTATIVE, B TITLE, C SIGNATURE, D GRADE, E DATE YYYYMMDD, DA FORM MAR, PREVIOUS EDITIONS ARE OBSOLETE, and Page of APD LC vES.
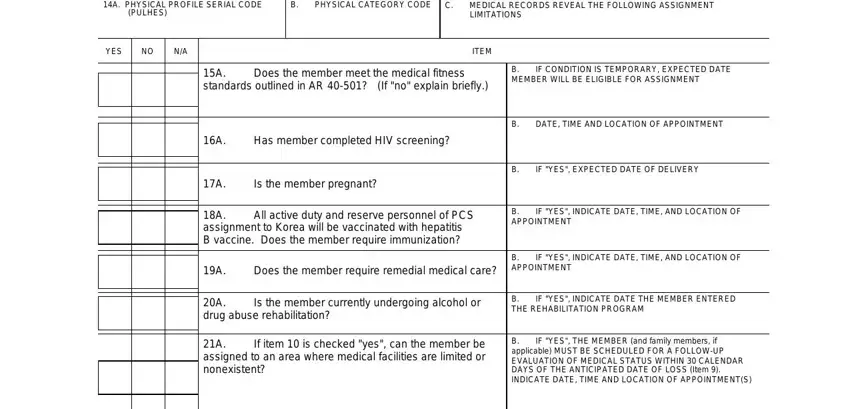
In the A PHYSICAL PROFILE SERIAL CODE, PULHES, YES, B PHYSICAL CATEGORY CODE, C MEDICAL RECORDS REVEAL THE, LIMITATIONS, ITEM, A Does the member meet the medical, B IF CONDITION IS TEMPORARY, A Has member completed HIV, A Is the member pregnant, A All active duty and reserve, B DATE TIME AND LOCATION OF, B IF YES EXPECTED DATE OF DELIVERY, and B IF YES INDICATE DATE TIME AND field, point out the key data.
The area REQUIRES, HAS, MISSING, ITEM, DATE TIME AND LOCATION OF, A Two pairs of spectacles, B Protective mask spectacle, insert, C Two hearing aids, D Medical warning tag, NAME OF MEDICAL OFFICER, B TITLE, SIGNATURE, D GRADE, and E DATE YYYYMMDD is going to be where to insert all parties' rights and obligations.
Terminate by taking a look at the following sections and completing them correspondingly: A If item is checked yes can the, B IF YES THE MEMBER and family, A NAME OF DENTAL OFFICER, B TITLE, C SIGNATURE, D GRADE, E DATE YYYYMMDD, DA FORM MAR, and Page of APD LC vES.
Step 3: Hit the Done button to be sure that your finished file is available to be exported to each gadget you end up picking or mailed to an email you specify.
Step 4: Make duplicates of the form. This may protect you from possible problems. We do not view or disclose your information, so be certain it will be secure.
Frequently Asked Questions about DA Form 4036
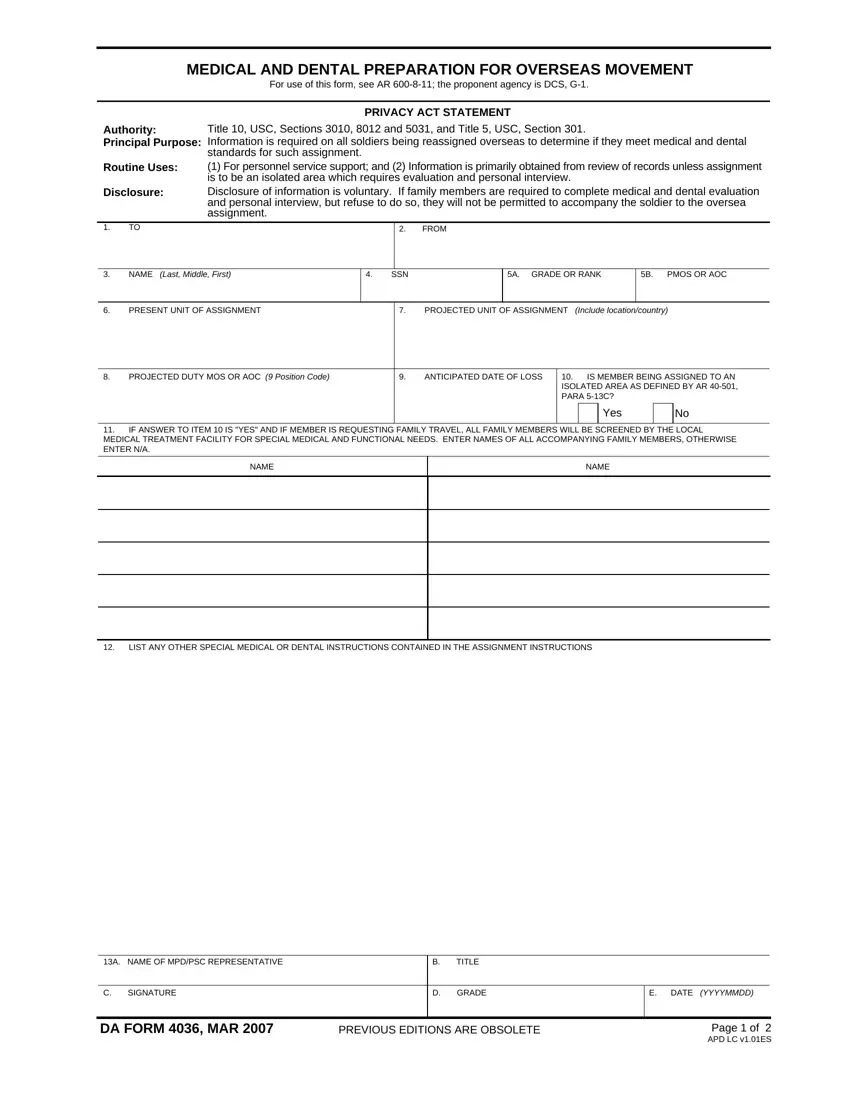
Who must complete this form?
Soldiers receiving overseas duty assignments under AR 600-8-11 must complete this form. Command-sponsored family members joining the soldier overseas are also screened.
When should the form be submitted?
Submit the completed form before your reporting date. Your unit S-1 or medical officer can advise on the exact deadline based on your gaining command’s requirements.
Does the form cover dental fitness?
Yes. The dental section certifies the soldier’s Class 1 or Class 2 dental readiness. Soldiers who do not meet dental standards are referred for treatment before departure.
Are there related forms I may need?
You may also need the DA Form 31 for leave requests and the SF 600 for your chronological medical record as part of the overseas clearance packet.
