
How to Fill Out DD Form 1952 Online
Use the FormsPal PDF editor to complete your DD Form 1952 online. No software download is needed. Follow the steps below to fill in your Dosimetry Application and Record of Previous Radiation Exposure quickly and correctly.
Step 1: Click the "Get Form" button at the top of this page to open the DD Form 1952 editor in your browser.
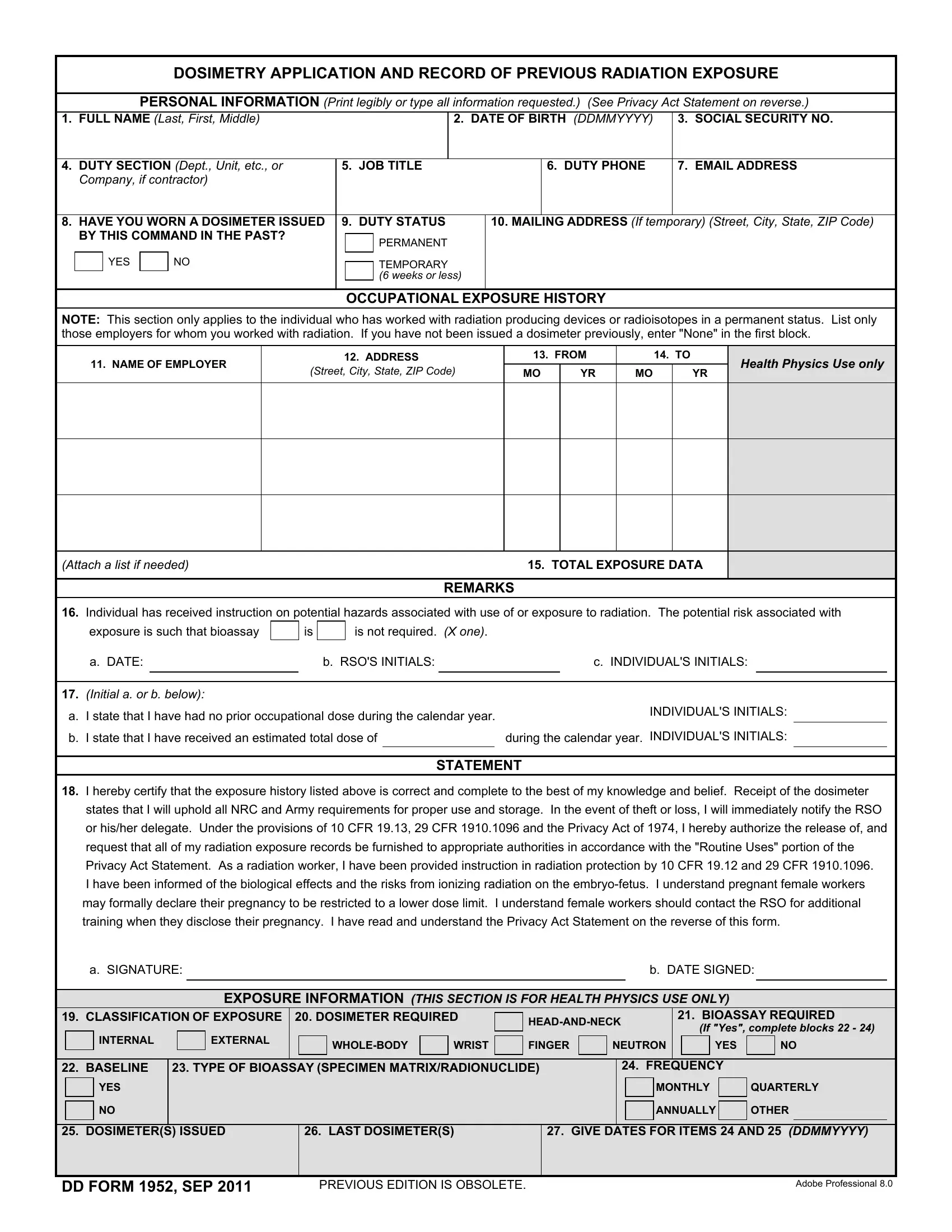
Step 2: Complete the personal information section at the top of the form. Enter your full name, date of birth, Social Security number, and current duty station. Double-check all entries for accuracy before moving on.
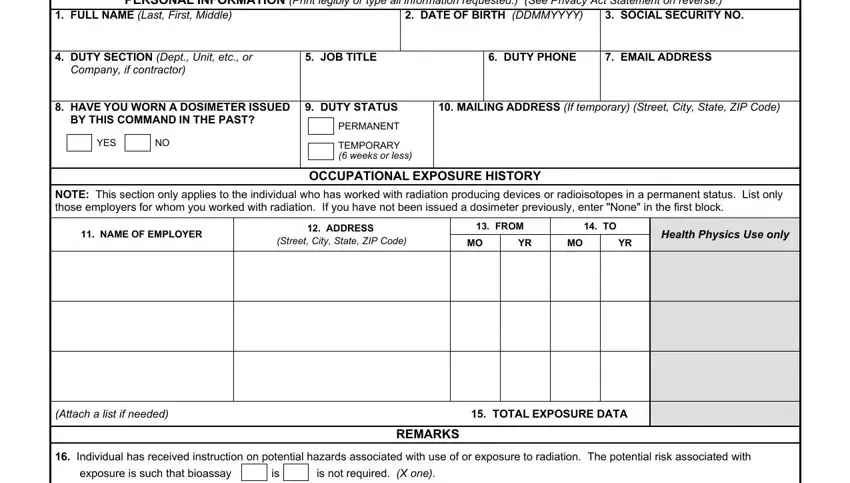
Step 3: Fill in the occupational exposure history section. Indicate whether you received a dosimeter from a previous command. If yes, enter the command name and the dates of service. This data helps your Radiation Safety Officer establish your cumulative dose record before issuing a new dosimeter.
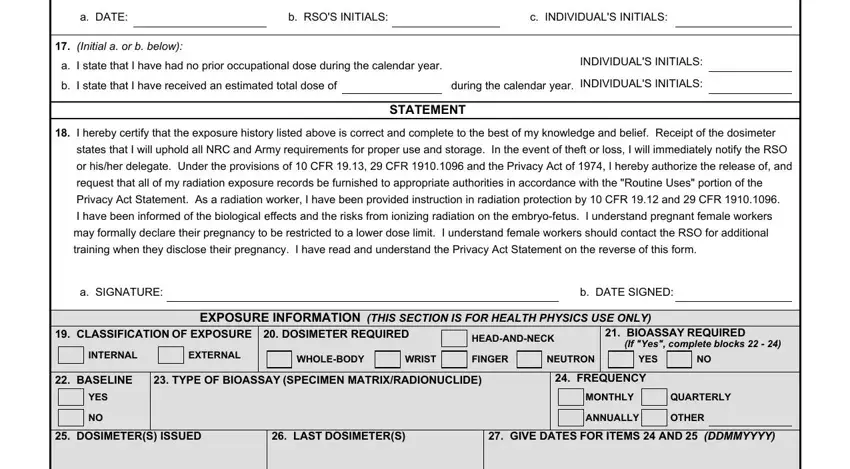
Step 4: Review and initial the compliance statement. Read each line of the Privacy Act statement carefully. Initial both options a and b as directed. Your initials confirm that you will follow all NRC and Army rules for dosimeter use, storage, and loss reporting.
Step 5: After reviewing all sections, click "Done" to finalize your form. Download the completed PDF and submit it to your unit's Radiation Safety Officer. Keep a copy for your personal records.
Common Questions About DD Form 1952
What information goes in the exposure history section?
You must state whether you received a dosimeter from a previous employer or military command. If yes, provide the organization name, dates of service, and the type of radiation work performed. If this is your first dosimeter assignment, you indicate no prior occupational radiation exposure.
What does the compliance statement require?
The statement requires you to confirm three things. First, you will use the dosimeter properly and return it as instructed. Second, you will store it away from heat, moisture, and background radiation sources. Third, you will report any loss or theft to your Radiation Safety Officer within the required time frame.
What happens after I submit the form?
Your Radiation Safety Officer reviews the form and enters your exposure data into the occupational exposure registry. You will then be issued a dosimeter suited to your assignment. Your records are maintained under Army Regulation 40-14 and are available for review at any time under the Privacy Act of 1974.
Related occupational health forms include the DD Form 2807-2 Medical Prescreening and the DD Form 2215 Reference Audiogram.