You can complete the de ins form illinois form with this PDF editor. These actions will assist you to immediately create your document.
Step 1: Select the "Get Form Now" button to get started on.
Step 2: Right now, you can change the de ins form illinois. The multifunctional toolbar will let you include, get rid of, change, highlight, and also perform several other commands to the text and areas inside the form.
Fill in the next areas to prepare the form:
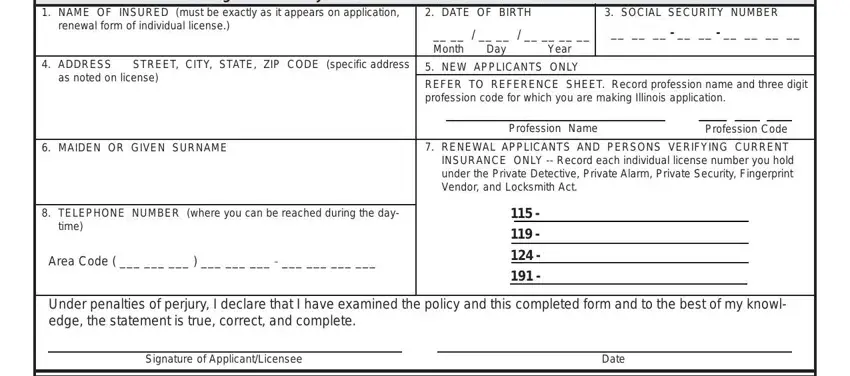
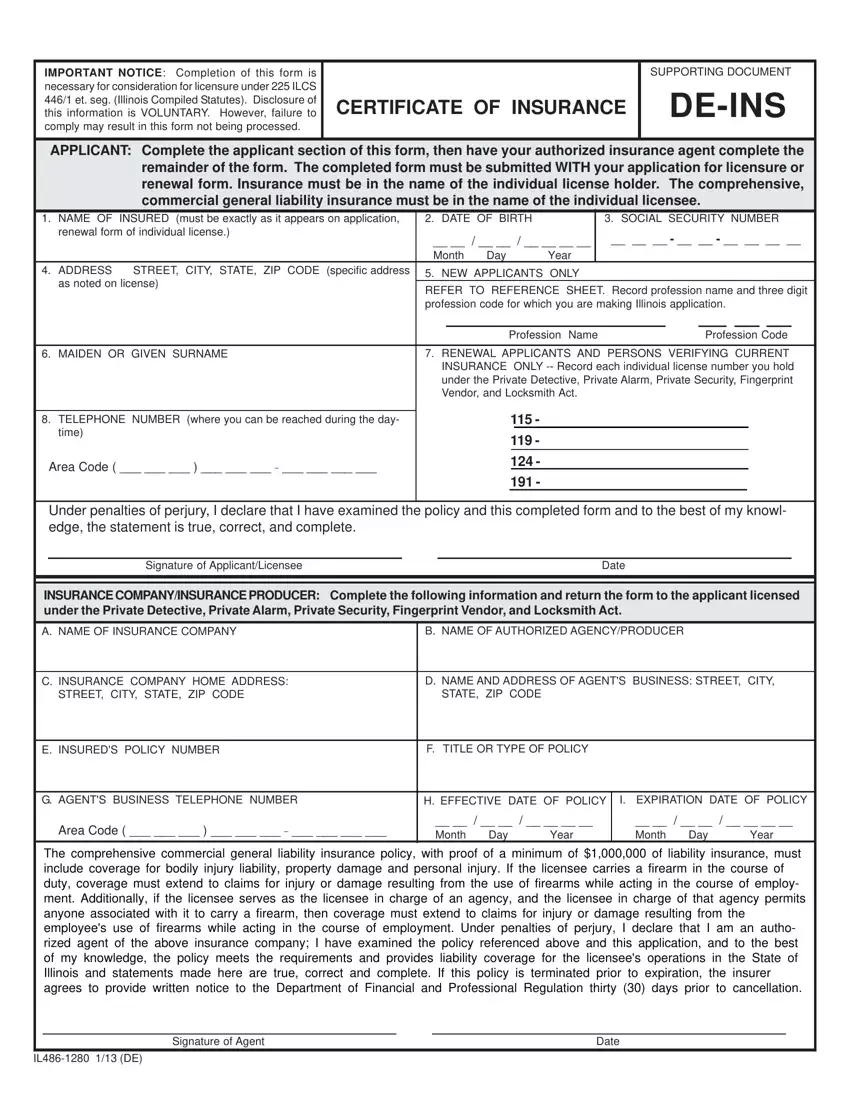
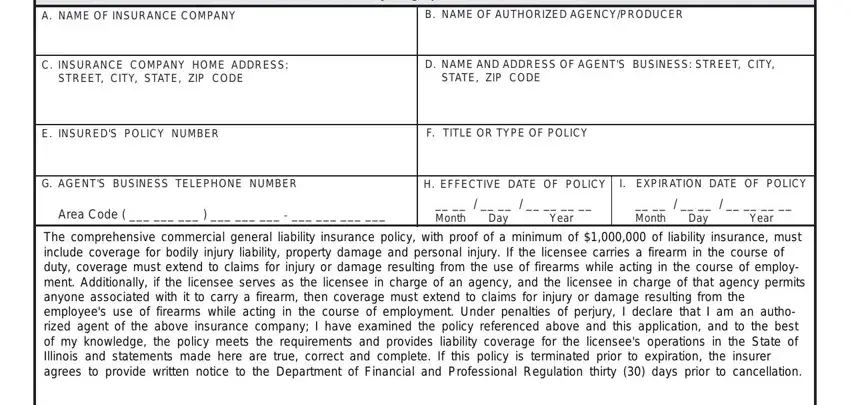
Complete the INSURANCE COMPANYINSURANCE, A NAME OF INSURANCE COMPANY, B NAME OF AUTHORIZED AGENCYPRODUCER, C INSURANCE COMPANY HOME ADDRESS, STREET CITY STATE ZIP CODE, D NAME AND ADDRESS OF AGENTS, STATE ZIP CODE, E INSUREDS POLICY NUMBER, F TITLE OR TYPE OF POLICY, G AGENTS BUSINESS TELEPHONE NUMBER, H EFFECTIVE DATE OF POLICY, I EXPIRATION DATE OF POLICY, Area Code, Month Day Year, and Month Day Year areas with any information that can be asked by the program.
Step 3: As soon as you are done, click the "Done" button to export your PDF document.
Step 4: To prevent yourself from any type of issues in the long run, you will need to prepare minimally several duplicates of your document.
