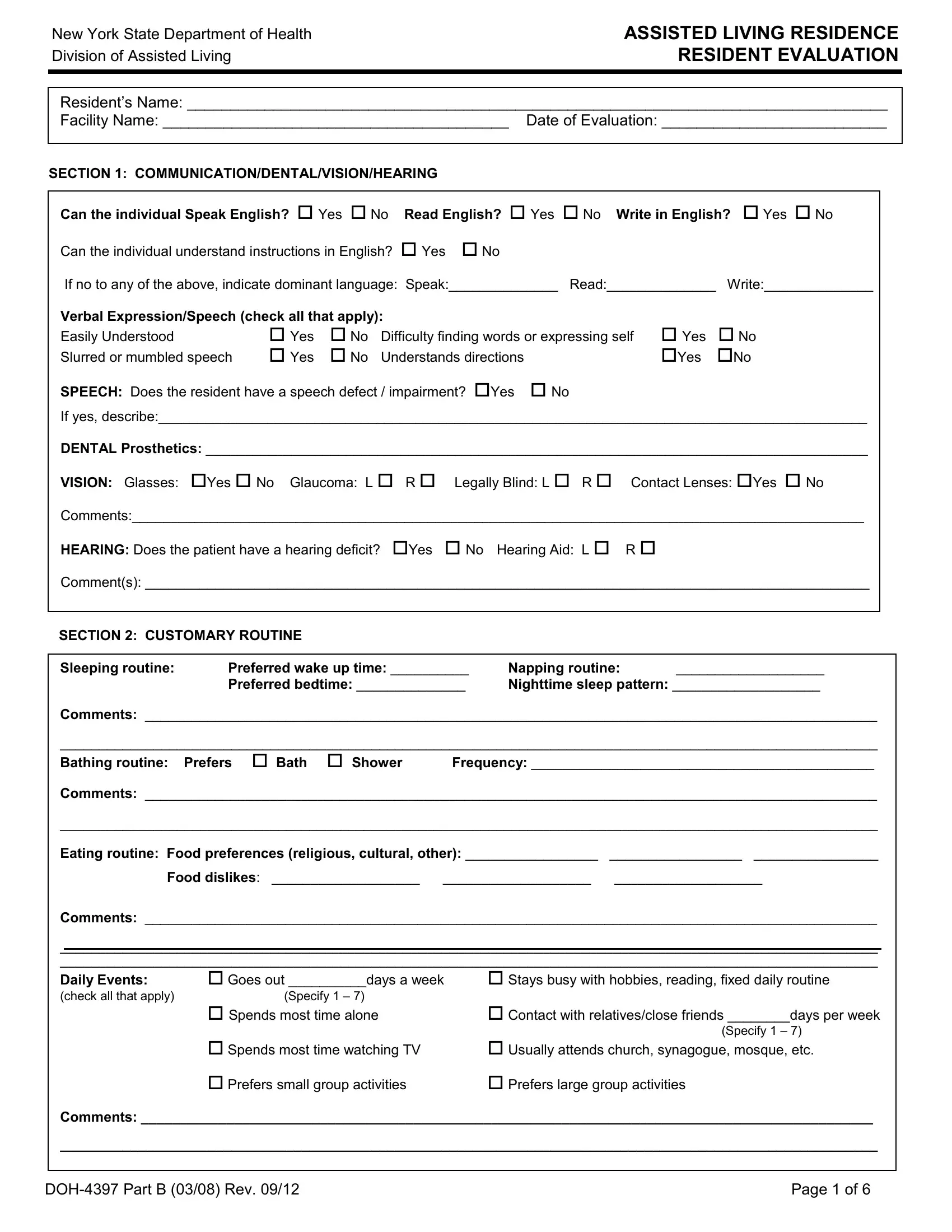
The New York State Department of Health's Division of Assisted Living has developed a comprehensive form known as DOH-4397, designed for the evaluation of residents in assisted living facilities. This form covers various aspects of a resident's health and daily living capabilities, aiming to provide a thorough assessment to ensure that individuals receive the appropriate level of care and support they need. It begins with assessing the resident's ability to communicate effectively in English, whether they can speak, read, write, and understand instructions, considering any speech impairments, dental, vision, and hearing issues they may have. Further, it delves into the resident's customary routine, including their sleeping, bathing, and eating habits, as well as their social activities and continence management. The form is detailed in its approach to evaluating physical functions, requiring information on the level of assistance needed for various tasks such as eating, ambulation, transferring, toileting, bathing, and dressing. Prosthetic needs, any podiatric concerns, and the resident’s ability to engage in housekeeping, shopping, and the use of a telephone are also examined. Additionally, the form screens for cognitive impairment, inquiring about the individual’s orientation, comprehension, concentration, memory, and any notable behaviors that could indicate cognitive decline. This evaluation instrument is critical for the tailored care planning and successful integration of residents into the assisted living community, ensuring their health, safety, and well-being are adequately addressed.
| Question | Answer |
|---|---|
| Form Name | Doh 4397 Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | 4397 b form, doh 4397, residence resident 1, nys doh 4397 form |

New York State Department of Health Division of Assisted Living
ASSISTED LIVING RESIDENCE RESIDENT EVALUATION
|
Resident’s Name: _________________________________________________________________________________ |
||||||||||||||
|
Facility Name: ________________________________________ |
Date of Evaluation: __________________________ |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
SECTION 1: COMMUNICATION/DENTAL/VISION/HEARING |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|||||||||||
|
Can the individual Speak English? Yes No |
Read English? Yes No |
Write in English? Yes No |
|
|
||||||||||
|
Can the individual understand instructions in English? |
Yes |
No |
|
|
|
|
|
|
||||||
|
If no to any of the above, indicate dominant language: Speak:______________ Read:______________ |
Write:______________ |
|
|
|||||||||||
|
Verbal Expression/Speech (check all that apply): |
|
|
|
|
|
|
|
|
|
|
||||
|
Easily Understood |
|
Yes |
No |
Difficulty finding words or expressing self |
Yes |
No |
|
|
||||||
|
Slurred or mumbled speech |
Yes |
No |
Understands directions |
|
|
Yes |
No |
|
|
|||||
|
SPEECH: Does the resident have a speech defect / impairment? Yes |
No |
|
|
|
|
|
||||||||
|
If yes, describe:___________________________________________________________________________________________ |
|
|
||||||||||||
|
DENTAL Prosthetics: _____________________________________________________________________________________ |
|
|
||||||||||||
|
VISION: Glasses: |
Yes No Glaucoma: L R |
|
Legally Blind: L R Contact Lenses: Yes No |
|
|
|||||||||
|
Comments:______________________________________________________________________________________________ |
|
|
||||||||||||
|
HEARING: Does the patient have a hearing deficit? |
Yes |
No |
Hearing Aid: L R |
|
|
|
|
|||||||
|
Comment(s): _____________________________________________________________________________________________ |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
SECTION 2: CUSTOMARY ROUTINE |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||||||||
|
Sleeping routine: |
Preferred wake up time: __________ |
Napping routine: |
___________________ |
|
|
|||||||||
|
|
Preferred bedtime: ______________ |
Nighttime sleep pattern: ___________________ |
|
|||||||||||
|
Comments: ______________________________________________________________________________________________ |
|
|||||||||||||
|
_________________________________________________________________________________________________________ |
|
|
||||||||||||
|
Bathing routine: |
Prefers |
Bath |
Shower |
|
Frequency: ____________________________________________ |
|
||||||||
|
Comments: ______________________________________________________________________________________________ |
|
|||||||||||||
|
_________________________________________________________________________________________________________ |
|
|
||||||||||||
|
Eating routine: Food preferences (religious, cultural, other): _________________ |
_________________ ________________ |
|
|
|||||||||||
|
Food dislikes: ___________________ |
___________________ |
___________________ |
|
|
||||||||||
|
Comments: ______________________________________________________________________________________________ |
|
|||||||||||||
|
_________________________________________________________________________________________________________ |
|
|
||||||||||||
|
_________________________________________________________________________________________________________ |
|
|
||||||||||||
|
Daily Events: |
Goes out __________days a week |
|
Stays busy with hobbies, reading, fixed daily routine |
|
||||||||||
|
(check all that apply) |
|
(Specify 1 – 7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spends most time alone |
|
|
|
|
Contact with relatives/close friends ________days per week |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
(Specify 1 – 7) |
|
|
|
|
Spends most time watching TV |
|
|
Usually attends church, synagogue, mosque, etc. |
|
|||||||||
|
|
Prefers small group activities |
|
|
Prefers large group activities |
|
|
|
|||||||
|
Comments: ______________________________________________________________________________________________ |
|
|||||||||||||
|
_________________________________________________________________________________________________________ |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Page 1 of 6 |
||||||

New York State Department of Health Division of Assisted Living
ASSISTED LIVING RESIDENCE RESIDENT EVALUATION
Resident’s Name: _________________________________________________________________________________
Facility Name: ________________________________________ Date of Evaluation: __________________________
SECTION 3: CONTINENCE STATUS/MANAGEMENT |
|
|
|
|
|
|
|
|
|||||||
Is the resident continent of urinary function? |
Yes |
No |
|
|
|
|
|
|
|
|
|||||
Is the resident continent of bowel function? |
Yes |
No |
|
|
|
|
|
|
|
|
|||||
IF ANSWER IS “NO” TO EITHER QUESTION, COMPLETE THIS SECTION, AS APPROPRIATE. |
|
|
|
||||||||||||
|
Urinary Incontinence |
|
|
|
|
Bowel Incontinence |
|
|
|||||||
|
Several times a week |
Day Only |
|
|
|
Several times a week |
|
Day only |
|
|
|||||
|
Daily |
|
|
Night only |
|
|
Daily |
|
|
|
Night only |
|
|
||
|
|
|
|
Day and night |
|
|
|
|
|
|
Day and night |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Current management techniques |
|
|
Current management techniques |
|
||||||||||
|
Prompting/reminding defers incontinence |
|
|
Uses incontinence pads/adult diapers: |
|
|
|
||||||||
|
Timed voiding defers incontinence |
|
|
|
Day only |
|
|
|
|
|
|
|
|||
|
Uses incontinence pads/adult diapers: |
|
|
|
Night only |
|
|
|
|
|
|
|
|||
|
Day only |
|
|
|
|
|
|
Day and night |
|
|
|
|
|
|
|
|
Night only |
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
Day and night |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__________________________________________________________ |
||||||||
|
Catheter (specify type) ____________________________ |
|
__________________________________________________________ |
||||||||||||
|
Comments: _____________________________________ |
|
__________________________________________________________ |
||||||||||||
_______________________________________________ |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
Yes No |
|
|
|||||||||
SECTION 4: PHYSICAL FUNCTION |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
TASK |
|
LEVEL OF ASSISTANCE |
|
|
|
|
COMMENTS |
|
|
|
||||
|
Eating: |
|
Independent: Able to feed self independently with or |
Dentures |
Upper |
Yes |
No |
||||||||
|
(Ability to feed self |
|
without assistive device. |
|
|
|
|
|
|
|
Lower |
Yes |
No |
||
|
meals and snacks) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Intermittent Assistance: Requires minimal, |
|
Chewing difficulties |
Yes |
No |
||||||||
|
|
|
intermittent supervision and/or assistance. |
|
|
|
|
|
|
|
|||||
|
|
|
Continual Assistance: Requires constant assistance |
|
Difficulty swallowing |
Yes |
No |
||||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
and/or supervision throughout meal. |
|
|
Modified consistency |
Yes |
No |
|||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
Total Assistance: Unable to feed self, needs to be fed. |
|
Specify ______________ |
|
|||||||||
|
|
|
|
Comments: |
|
|
|
||||||||
|
|
|
Unable to take nutrients orally, requires enteral nutrition. |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
||||||||
|
Ambulation: |
|
Independent: Walks and climbs and descends stairs |
|
Wheelchair |
Walker |
|
||||||||
|
(Ability to safely walk |
|
independently with or without assistive device. |
|
|
|
|
|
|
|
|||||
|
and move about once |
|
|
|
|
|
|
|
|
Quad cane |
Cane |
|
|||
|
in a standing position) |
|
Intermittent Assistance: Walks and climbs and |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
descends stairs with minimal, intermittent assistance |
|
Other: ____________________ |
||||||||||
|
|
|
and/or supervision. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Continual Assistance: Walks and climbs and |
|
Falls within the last 3 months? |
|
|||||||||
|
|
|
|
|
|
Yes No |
|
||||||||
|
|
|
descends stairs with constant supervision and/or |
|
Frequency #: _______________________ |
||||||||||
|
|
|
assistance. |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Total Assistance: Chairfast or bedfast. Requires total |
|
Injury: ____________________________ |
||||||||||
|
|
|
|
Comments: |
|
|
|
||||||||
|
|
|
assistance for mobility. |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
Page 2 of 6 |
||||||
New York State Department of Health Division of Assisted Living
ASSISTED LIVING RESIDENCE RESIDENT EVALUATION
Resident’s Name: _________________________________________________________________________________
Facility Name: ________________________________________ Date of Evaluation: __________________________
|
TASK |
|
|
LEVEL OF ASSISTANCE |
|
|
COMMENTS |
|
Transferring: |
|
|
Independent: Able to transfer independently with or |
|
|
Comments: |
|
(Moving from bed to |
|
|
without assistive device. |
|
|
|
|
chair, on/off toilet, |
|
|
|
|
|
|
|
in/out of shower or |
|
|
Intermittent Assistance: Transfers with minimal |
|
|
|
|
tub) |
|
|
|
|
|
|
|
|
|
human assistance and/or supervision. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Continual Assistance: Unable to transfer but can bear |
|
|
|
|
|
|
|
weight and pivot when transferred by at least one other |
|
|
|
|
|
|
|
person. |
|
|
|
|
|
|
|
Total Assistance: Chairfast or bedfast, unable to |
|
|
|
|
|
|
|
transfer, pivot, bear weight or turn self in bed. |
|
|
|
PROSTHESIS: No Yes (describe)__________________________________________________________________________
AMPUTATION: No Yes (describe)___________________________________________________________________________
PODIATRIC: Does the resident have podiatric concerns requiring treatment or which impair ability to ambulate or transfer? No Yes (describe)_______________________________________________________________________________
|
|
|
|
|
|
|
|
|
|
TASK |
|
|
LEVEL OF ASSISTANCE |
|
|
COMMENTS |
|
|
Toileting: (Getting to/from |
|
|
Independent: Able to toilet independently with or without |
|
|
Ostomy |
Yes No |
|
and on/off the toilet, |
|
|
assistive device. |
|
|
Comments: |
|
|
cleansing self after |
|
|
Intermittent Assistance: Able to toilet with minimal |
|
|
|
|
|
|
|
|
|
|
|
||
|
elimination and adjusting |
|
|
intermittent assistance and/or supervision. |
|
|
|
|
|
clothing) |
|
|
|
|
|
|
|
|
|
|
Continual Assistance: Able to toilet with constant |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
assistance and/or supervision. |
|
|
|
|
|
|
|
|
Total Assistance: Unable to toilet. Requires total |
|
|
|
|
|
|
|
|
assistance with toileting. |
|
|
|
|
|
Bathing: (Getting in and |
|
|
Independent: Able to bathe or shower independently with |
|
|
Comments: |
|
|
out of tub or shower, |
|
|
or without assistive device. |
|
|
|
|
|
washing and drying entire |
|
|
|
|
|
|
|
|
|
|
Intermittent Assistance: Able to bathe or shower |
|
|
|
|
|
|
body) |
|
|
w/minimal intermittent assistance and/or supervision. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Continual Assistance: Able to bathe or shower with |
|
|
|
|
|
|
|
|
constant assistance and/or supervision. |
|
|
|
|
|
|
|
|
Total Assistance: Unable to use shower or tub. Bathed |
|
|
|
|
|
|
|
|
in bed or at bedside. |
|
|
|
|
|
Dressing: (Getting clothes |
|
|
Independent: Able to dress and undress independently |
|
|
Comments: |
|
|
from closets and drawers, |
|
|
with or without assistive device. |
|
|
|
|
|
dressing and undressing |
|
|
|
|
|
|
|
|
|
|
Intermittent Assistance: Able to dress and undress with |
|
|
|
|
|
|
upper/lower body including |
|
|
|
|
|
|
|
|
buttons, snaps, zippers, |
|
|
minimal, intermittent assistance and/or supervision. |
|
|
|
|
|
|
|
Continual Assistance: Requires assistance throughout |
|
|
|
|
|
|
socks and shoes) |
|
|
|
|
|
|
|
|
|
|
|
the dressing and undressing process. |
|
|
|
|
|
|
|
|
Total Assistance: Requires another person to dress and |
|
|
|
|
|
|
|
|
undress upper and lower body. |
|
|
|
|
|
|
|
|
Page 3 of 6 |
||||

New York State Department of Health Division of Assisted Living
ASSISTED LIVING RESIDENCE RESIDENT EVALUATION
Resident’s Name: _________________________________________________________________________________
Facility Name: ________________________________________ Date of Evaluation: __________________________
|
SECTION 4: PHYSICAL FUNCTION Cont. |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
TASK |
|
|
LEVEL OF ASSISTANCE |
COMMENTS |
|
Grooming: (Washing face, |
|
|
Independent: Able to groom self independently with or |
Comments: |
|
hair care, shaving, |
|
|
without assistive device. |
|
|
teeth/denture, fingernail |
|
|
|
|
|
|
|
Intermittent Assistance: Requires grooming utensils to |
|
|
|
care, eyeglasses care) |
|
|
|
|
|
|
|
be set up and placed within reach. |
|
|
|
|
|
|
|
|
|
|
|
|
Continual Assistance: Requires assistance throughout |
|
|
|
|
|
the grooming process. |
|
|
|
|
|
Total Assistance: Depends entirely upon someone else |
|
|
|
|
|
for grooming. |
|
|
Transportation: (Physical |
|
|
Independent: Able to independently drive a regular or |
Comments: |
|
and mental ability to safely |
|
|
adapted car; OR uses a regular or handicap accessible public |
|
|
use a car, taxi, or public |
|
|
|
|
|
|
bus, train or subway. |
|
||
|
transportation [bus, train, |
|
|
||
|
|
|
Independent: But requests facility perform task. |
|
|
|
subway) |
|
|
|
|
|
|
|
Intermittent Assistance: Able to ride in a car only when |
|
|
|
|
|
|
|
|
|
|
|
|
driven by another person; AND/OR due to physical, cognitive |
|
|
|
|
|
or mental limitations occasionally requires another person to |
|
|
|
|
|
accompany him/her when using a bus, train or subway. |
|
|
|
|
|
Continual Assistance: Able to ride in a car only when |
|
|
|
|
|
driven by another person; OR able to use a bus or handicap |
|
|
|
|
|
van, train or subway only when assisted or accompanied by |
|
|
|
|
|
another person. |
|
|
|
|
|
Total Assistance: Unable to ride in a car, taxi, bus or |
|
|
|
|
|
van, and requires transportation by ambulance. |
|
|
Laundry: (Ability to do own |
|
|
Independent: Able to independently take care of all |
Comments: |
|
laundry – to carry laundry |
|
|
laundry tasks. |
|
|
to and from washing |
|
|
|
|
|
|
|
Independent: But requests facility perform task. |
|
|
|
machine, to use washer |
|
|
|
|
|
|
|
Intermittent Assistance: Able to do only light laundry, |
|
|
|
and dryer, to wash small |
|
|
|
|
|
items by hand) |
|
|
such as minor hand wash or light washer loads. Needs |
|
|
|
|
|
assistance with heavy laundry, such as carrying large loads |
|
|
|
|
|
of laundry. |
|
|
|
|
|
Continual Assistance: Due to physical, cognitive or |
|
|
|
|
|
mental limitations, needs continual supervision and |
|
|
|
|
|
assistance to do any laundry. |
|
|
|
|
|
Total Assistance: Unable to do any laundry. |
|
|
|
|
|
|
|
|
Housekeeping: (Ability to |
|
|
Independent: Able to independently perform all |
Comments: |
|
safely and effectively |
|
|
housekeeping tasks. |
|
|
perform light housekeeping |
|
|
|
|
|
|
|
Independent: But requests facility perform task. |
|
|
|
and heavier cleaning tasks) |
|
|
Intermittent Assistance: Able to perform only light |
|
|
|
|
|
housekeeping (e.g., dusting, wiping kitchen counters) tasks |
|
|
|
|
|
independently; AND/OR able to perform housekeeping tasks |
|
|
|
|
|
with intermittent assistance or supervision from another |
|
|
|
|
|
person. |
|
|
|
|
|
Continual Assistance: Unable to consistently perform |
|
|
|
|
|
any housekeeping tasks unless assisted by another person |
|
|
|
|
|
throughout the process. |
|
|
|
|
|
Total Assistance: Unable to effectively participate in any |
|
|
|
|
|
housekeeping tasks. |
|
Page 4 of 6 |
New York State Department of Health Division of Assisted Living
ASSISTED LIVING RESIDENCE RESIDENT EVALUATION
Resident’s Name: _________________________________________________________________________________
Facility Name: ________________________________________ Date of Evaluation: __________________________
SECTION 4: PHYSICAL FUNCTION cont.
|
TASK |
|
|
LEVEL OF ASSISTANCE |
|
|
COMMENTS |
|
|
|
|
|
|
|
|
|
Shopping: (Ability to |
|
|
Independent: Able to plan for shopping needs and independently |
|
|
Comments: |
|
plan form, select and |
|
|
perform shopping tasks, including carrying package. |
|
|
|
|
purchase items in a |
|
|
|
|
|
|
|
|
|
Independent: But requests facility perform task. |
|
|
|
|
|
store and to carry them |
|
|
|
|
|
|
|
home or arrange |
|
|
Intermittent Assistance: Able to do only light shopping and carry |
|
|
|
|
delivery) |
|
|
small packages, but needs someone to do occasional major shopping. |
|
|
|
|
|
|
|
Continual Assistance: Unable to go shopping alone, but can go |
|
|
|
|
|
|
|
with someone to assist; OR unable to go shopping but is able to |
|
|
|
|
|
|
|
identify items needed, place orders, and arrange for home delivery. |
|
|
|
|
|
|
|
Total Assistance: Needs someone to do all shopping and |
|
|
|
|
|
|
|
errands. |
|
|
|
|
Ability to use a |
|
|
Independent: Able to dial numbers and answers calls |
|
|
Comments: |
|
Telephone: (Ability to |
|
|
appropriately and as desired. |
|
|
|
|
|
|
|
|
|
|
|
|
answer the telephone, |
|
|
Independent: But requests facility perform task. |
|
|
|
|
dial numbers, and |
|
|
Intermittent Assistance: Able to use a specially adapted |
|
|
|
|
effectively use the |
|
|
|
|
|
|
|
|
|
telephone (i.e., large numbers on the dial pad, teletype phone for the |
|
|
|
|
|
telephone to |
|
|
|
|
|
|
|
|
|
deaf) and call essential numbers; able to answer the telephone and |
|
|
|
|
|
communicate) |
|
|
|
|
|
|
|
|
|
carry on a normal conversation but has difficulty with placing calls; |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
able to answer the telephone only some of the time or is able to carry |
|
|
|
|
|
|
|
on only a limited conversation. |
|
|
|
|
|
|
|
Continual Assistance: Unable to make calls or answer the |
|
|
|
|
|
|
|
telephone at all, but can listen if assisted with equipment. |
|
|
|
|
|
|
|
Total Assistance: Totally unable to use the telephone. Requires |
|
|
|
|
|
|
|
someone else to make calls. |
|
|
|
|
|
|
|
|
|
|
|
SECTION 5: COGNITIVE IMPAIRMENT SCREEN
Cognitive Functioning: Individual’s current level of alertness, orientation, comprehension, concentration and immediate memory.
Response: What is today’s date? |
Correct |
Incorrect |
What day of the week is today: |
(correct, if within 2 days) |
|
|
|
How old are you? |
Correct |
Incorrect |
When were you born? |
Correct
Correct
Incorrect
Incorrect
Behaviors of Note: (check all that apply): |
|
Wanders Day/Night Sleep disturbance Confused Depressive Feelings Anxious |
Withdrawn/Refuses to Socialize |
Agitated (repeated vocalizations, screaming, shouting, moaning, cursing, fidgeting, etc.) |
Other:____________________ |
Overall Cognitive Functioning:(check all that apply):
Is alert and oriented, comprehends verbal questions and commands and has accurate recall
Requires prompting and redirection, on occasion, to complete tasks
Has occasional fluctuation in orientation, memory/alertness
Has significant memory loss and is disoriented to person, place and/or time
This screen includes indicators, which are often related to cognitive impairment. This is a screen ONLY and is intended to assist the residence in determining if an individual is appropriate for care in an ALR and/or if the individual should be referred to his/her physician for consultation and/or further evaluation or treatment.
Comments: _______________________________________________________________________________________________
_________________________________________________________________________________________________________
_________________________________________________________________________________________________________
Page 5 of 6 |