Filling out texas form 3643 department aging is simple. Our team developed our PDF software to make it simple to use and enable you to fill out any PDF online. Here are a few steps you need to follow:
Step 1: Choose the "Get Form Here" button.
Step 2: Now you may modify your texas form 3643 department aging. Feel free to use our multifunctional toolbar to add, remove, and change the content material of the document.
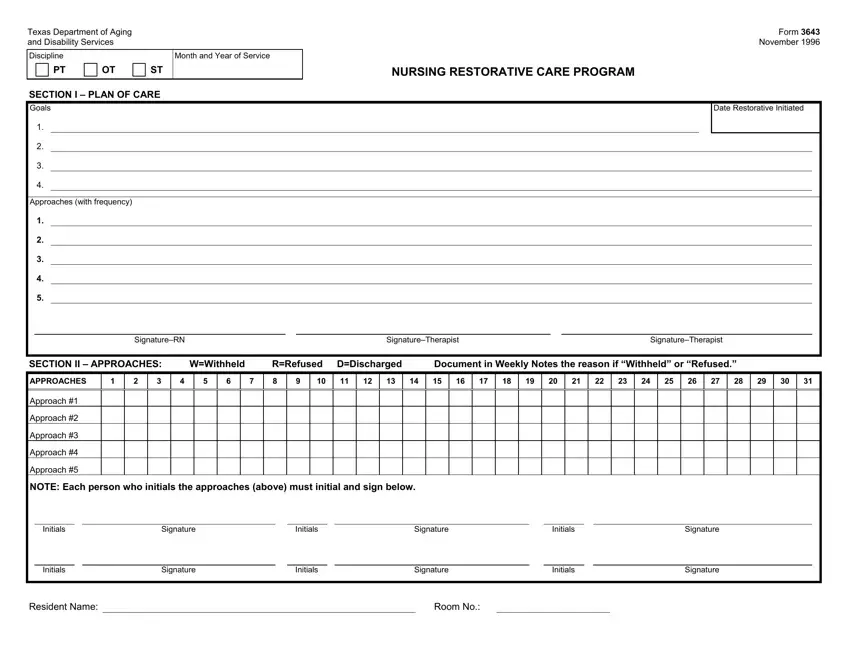
Complete the texas form 3643 department aging PDF by providing the data meant for each section.
In the APPROACHES, Approach, Approach, Approach, Approach, Approach, NOTE Each person who initials the, Initials, Signature, Initials, Signature, Initials, Signature, Initials, and Signature box, put down your data.
The application will ask for additional information as a way to instantly prepare the field Week Response, Week Response, Week Response, Week Response, Signature, Date, Signature, Date, Signature, Date, Signature, and Date.
Please make sure to include the rights and responsibilities of the sides inside the Week Response, Signature, Date, SECTION IV MONTHLY REVIEW, Is the Plan of Care appropriate, B Are changes to the Restorative, Are changes recommended to the, Are changes recommended to the, If YES to any items in B update, Comments, Yes Yes Yes Yes, and No No No No section.
Review the areas C Continue Program, Yes, D Discharge to basic nursing, Yes, SignatureLicensed Staff, and Date and then complete them.
Step 3: Hit the "Done" button. Now it's easy to transfer your PDF form to your electronic device. Additionally, you can easily forward it via email.
Step 4: Be sure to make as many copies of the file as possible to remain away from potential misunderstandings.
