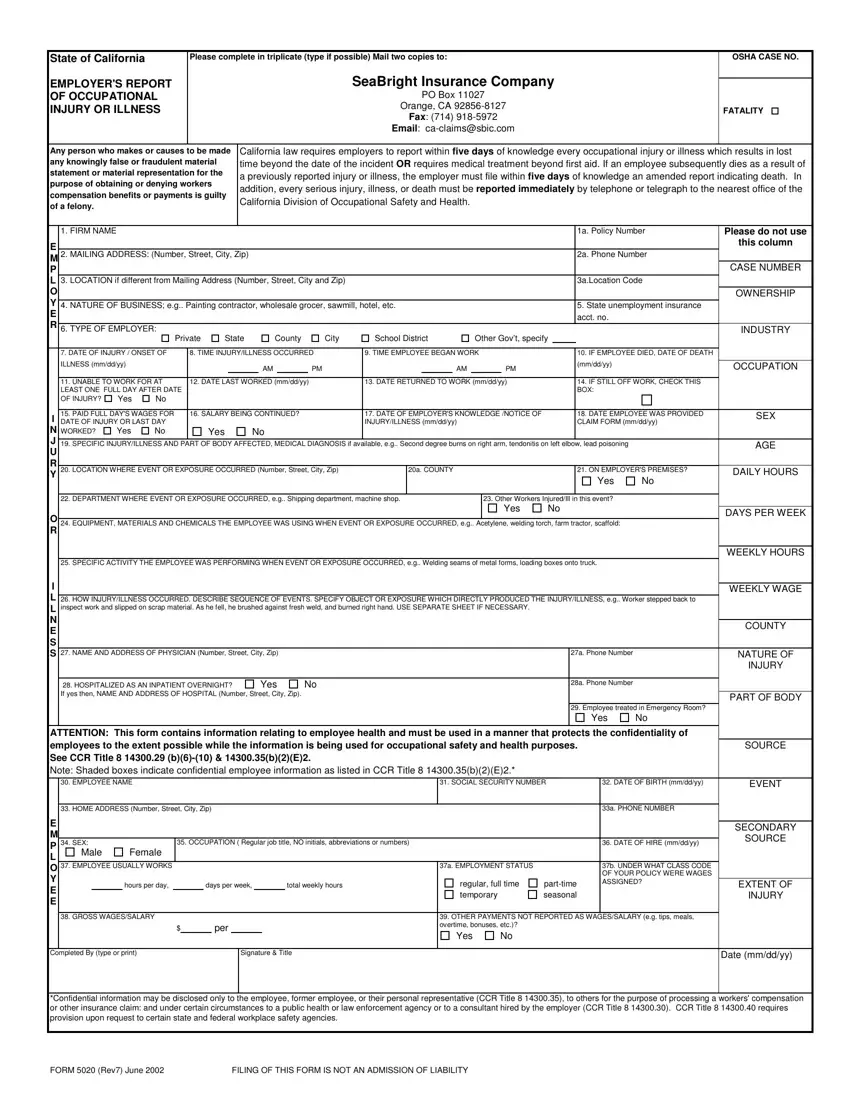
Navigating the complexities of workplace safety obligations, the 5020 California Form stands as a critical document for employers within the state, encapsulating the stringent reporting requirements set forth by California law. This form, known as the Employer's Report of Occupational Injury or Illness, must be completed meticulously and submitted promptly—within five days when an occupational injury or illness results in lost time beyond the day of the incident or necessitates medical treatment beyond first aid. The form plays a key role in the realm of workers' compensation, providing crucial details such as the nature of the business, specifics of the injury or illness, and the circumstances under which the event occurred. It underscores the legal mandate for immediate reporting to the California Division of Occupational Safety and Health in cases of severe injuries, illnesses, or death. Compliance with this requirement not only aids in the facilitation of workers' compensation benefits but also serves as a measure of prevention and correction, ensuring a safer workplace environment. Employers are reminded of the severe implications for knowingly making false or fraudulent statements related to workplace injuries, illustrating the form's pivotal role in maintaining transparency and accountability. Additionally, its proviso of information regarding employee confidentiality highlights a careful balance between occupational safety and employee privacy. The 5020 Form embodies the shared responsibility between employers and regulatory bodies to uphold worker health and safety as paramount.
| Question | Answer |
|---|---|
| Form Name | Form 5020 California |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 33a, po box 11027 orange ca, false, seabright insurance po box 11027 |
