
The CDCR 106 A form is a one-page fillable PDF with 53 fields. Complete the form and mail it to the Litigation Coordinator's office at the inmate's correctional institution. The California Department of Corrections and Rehabilitation (CDCR) will review the request before granting confidential phone access.
Information Required to Complete the CDCR 106 A Form
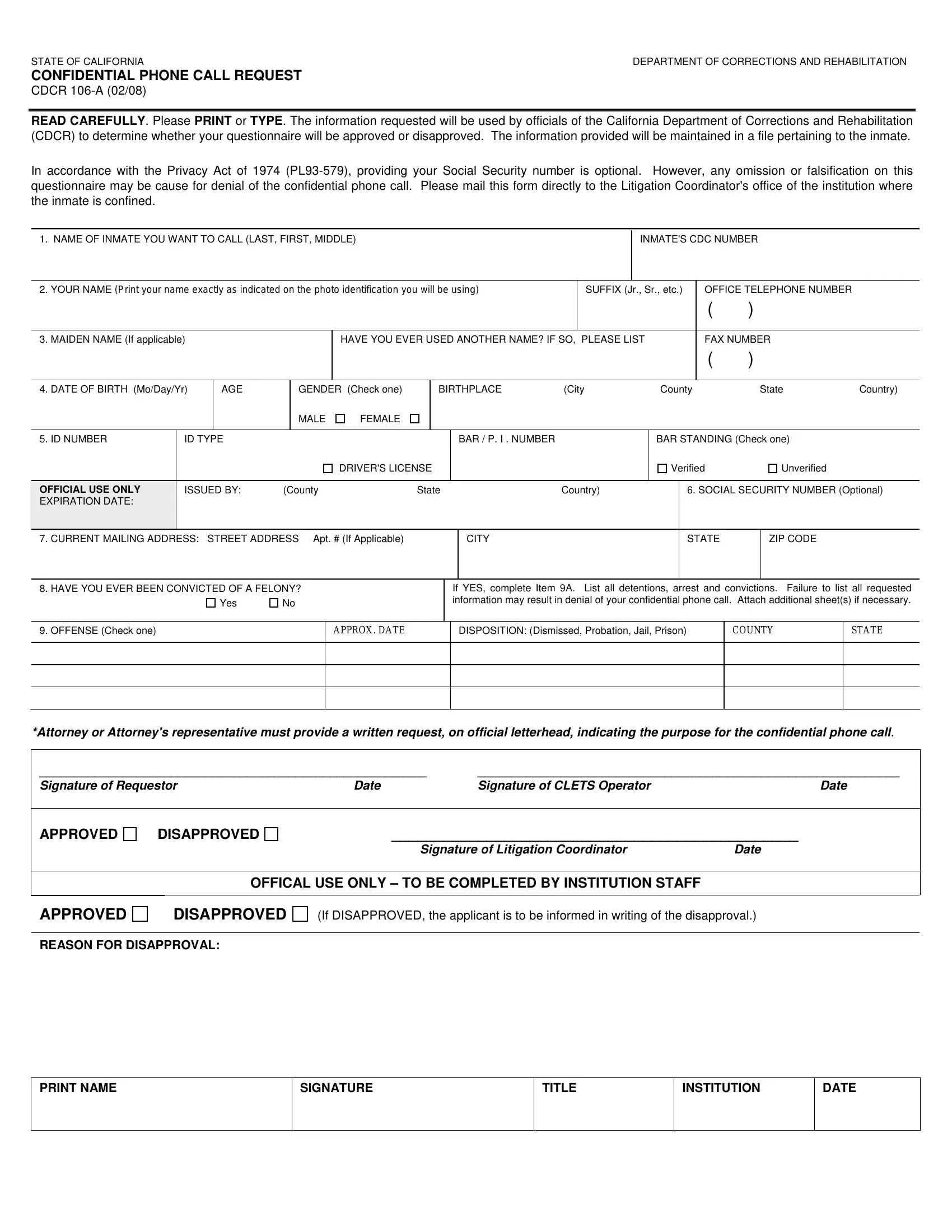
Gather the following information before filling out the CDCR 106 A form PDF:
- Requester details: Full legal name, mailing address, phone number, and relationship to the inmate
- Inmate information: Full name, CDC number, and the name of the CDCR correctional institution where the inmate is housed
- Attorney or representative information: State bar number and contact details if submitting on behalf of an attorney or legal representative
- Felony conviction history: Accurate disclosure of any prior felony convictions as required under the Privacy Act of 1974 (PL 93-579)
- Purpose of the request: A written statement explaining the need for confidential phone communication with the inmate
How to Fill Out the CDCR 106 A Form Step by Step
- Open the CDCR 106 A form PDF using the button at the top of this page to access the online editor.
- Enter the inmate's full name, CDC number, and the name of the CDCR facility where they are currently housed.
- Provide your full legal name, current mailing address, phone number, and your relationship to the inmate.
- Complete the felony conviction disclosure section honestly. Falsification of information leads to automatic denial of the confidential phone call request.
- If you are an attorney or legal representative, include a written statement confirming your state bar number and the legal purpose of the communication.
- Review all 53 fields to confirm that the form is complete and accurate before printing.
- Print the completed CDCR 106 A form and sign it where required.
- Mail the signed form to the Litigation Coordinator's office at the inmate's CDCR institution.
How to Submit the Completed CDCR 106 A Form
The CDCR 106 A form must be submitted by mail to the Litigation Coordinator's office at the specific CDCR correctional facility where the inmate is housed. There is no online submission option for this form. Allow adequate time for CDCR officials to process and evaluate each request for confidential phone communication.
Frequently Asked Questions About the CDCR 106 A Form
What is the CDCR 106 A form used for?
The CDCR 106 A form is an official California Department of Corrections and Rehabilitation document used to request confidential phone call access to inmates in state correctional facilities. It allows attorneys and other authorized individuals to communicate privately with an incarcerated person.
Who can submit the CDCR 106 A form?
Attorneys, legal representatives, and other authorized parties may submit the CDCR 106 A form. All requesters must provide accurate personal information and disclose any prior felony convictions under PL 93-579.
What happens after the CDCR 106 A form is submitted?
After CDCR officials receive the completed form, they review the request and evaluate whether the conditions for confidential phone communication are met. The Litigation Coordinator's office will notify the requester of the decision.
What causes the CDCR 106 A form to be denied?
Common reasons for denial include falsification of information, undisclosed felony convictions, incomplete fields, or failure to include the required written statement from an attorney. Accurate and complete disclosure is critical to having the form approved.
Related CDCR PDF Forms
These CDCR forms are commonly needed alongside the CDCR 106 A form:
- CDCR 602 Form – Used to file inmate appeals and grievances within the California correctional system
- CDCR 1824 Form – Reasonable modification or accommodation request for incarcerated individuals
- CDCR 7385 Form – Rehabilitation programming and participation documentation
- CDCR 1707 Form – Additional CDCR correspondence and documentation form
- CDCR 2152 Form – California Department of Corrections documentation form