It won't be a challenge to obtain nephrologist using our PDF editor. Here's how you may easily develop your document.
Step 1: Click the "Get Form Here" button.
Step 2: After you've entered the nephrologist edit page, you'll see all actions you may use with regards to your file at the upper menu.
Enter the necessary details in every single segment to create the PDF nephrologist
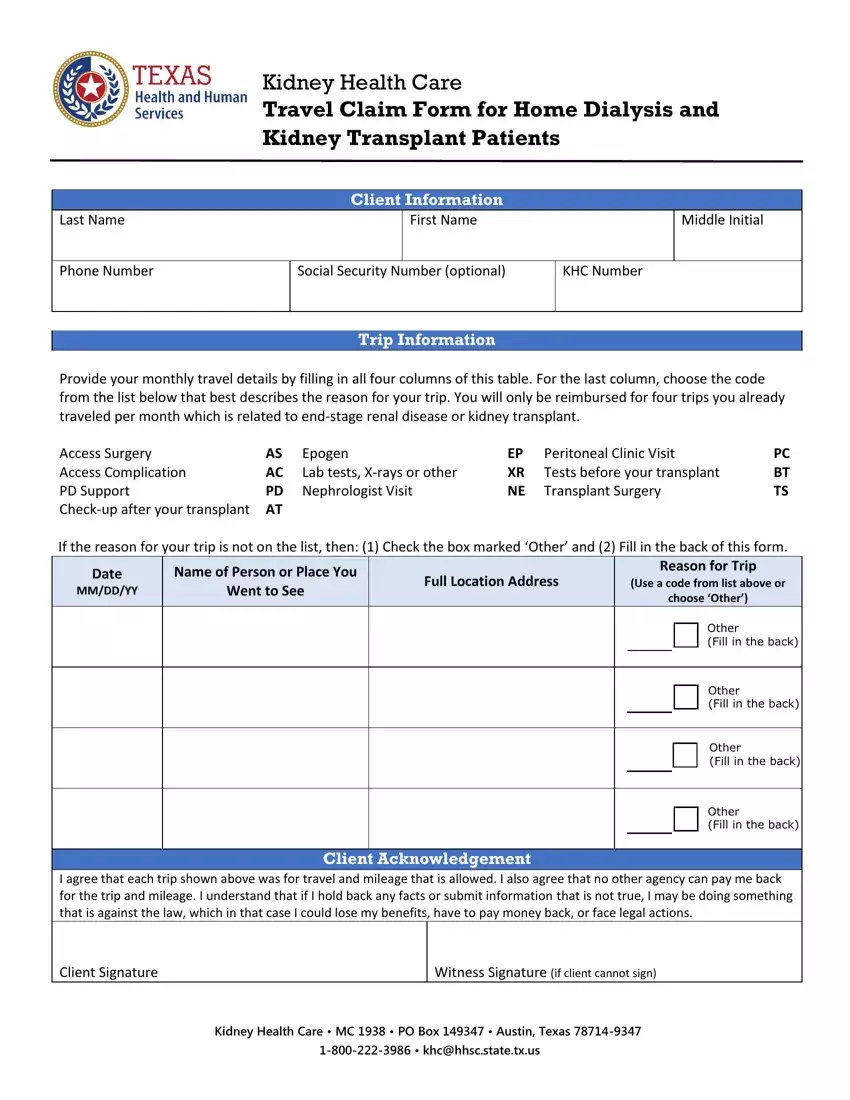
Write the information in Other Fill in the back, Other Fill in the back, Other Fill in the back, Client Acknowledgement I agree, Client Signature, Witness Signature if client cannot, Kidney Health Care MC PO Box, and khchhscstatetxus.
In the If KHC has already reviewed and, Date of Trips, Where did you go Place or Doctors, and Describe how the trip is related part, point out the relevant data.
Make sure you write down the rights and responsibilities of the parties inside the KHC will do a medical review with, For Use By KHC Reviewer ONLY, Comments, Date, Allow Trips, Disallow Trips, and Notice about Your Right to Privacy space.
Step 3: Select the "Done" button. Now you can export your PDF document to your electronic device. Additionally, it is possible to send it through electronic mail.
Step 4: Generate duplicates of the document - it will help you prevent forthcoming difficulties. And don't worry - we don't publish or see your data.
