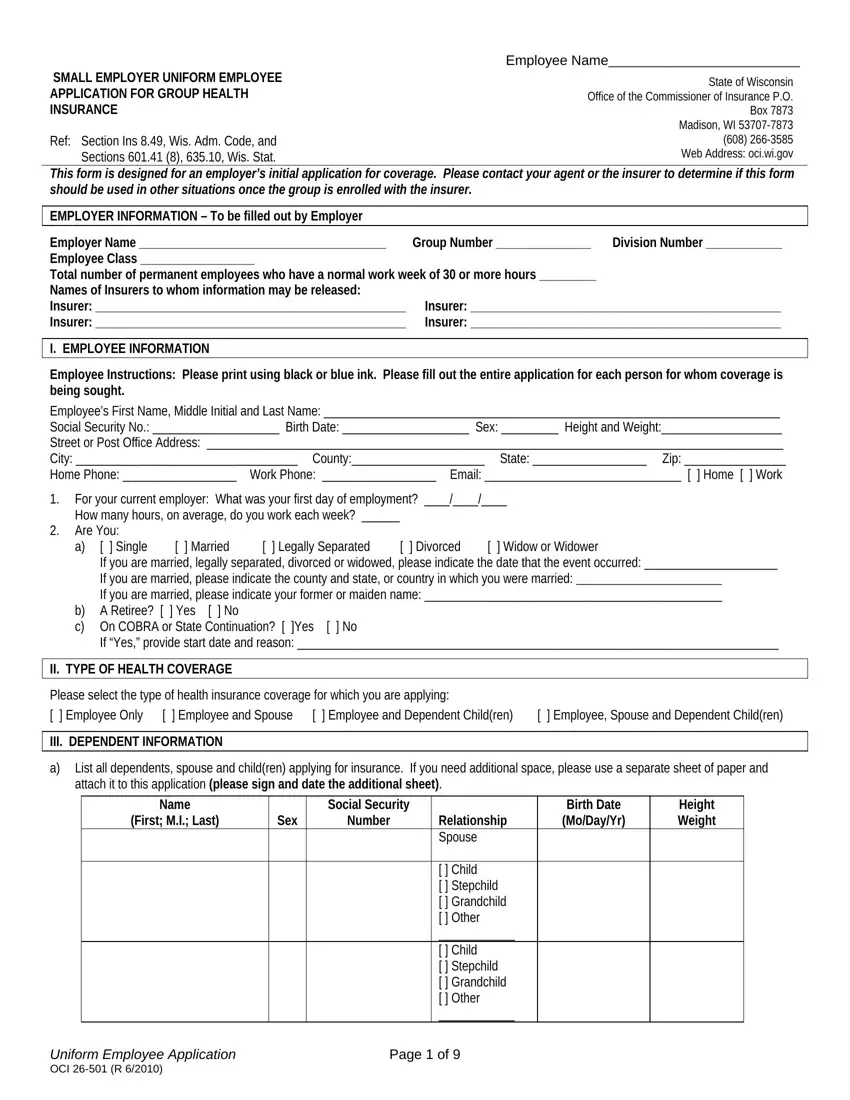
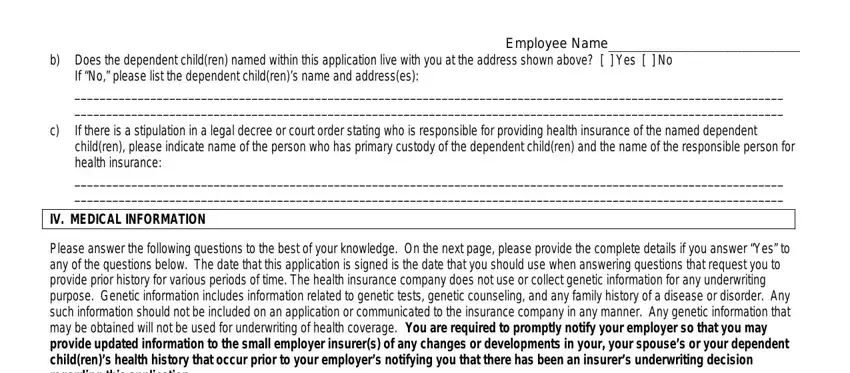
Employee Name_______________________
AUTHORIZATION TO USE AND DISCLOSE PROTECTED HEALTH INFORMATION
Instructions: Please read this authorization form carefully before signing. This form must be signed by each adult person seeking coverage, including all adult dependent children. Parents should sign for their minor children unless the minor has received treatment without parental consent, consistent with state law. Your application cannot be processed without a signature for each person seeking coverage. Signing this form is a condition of coverage: if you decide not to sign, you will not be enrolled in a health plan of the insurers listed below. You have the right to receive a copy of this form following your signature.
I. Protected Health Information
By signing this form, I authorize certain organizations and persons to use or disclose my, my spouse’s and my dependent child(ren)’s protected health information. Protected health information includes, but is not limited to, hospital records, physician records, lab results, mental health records, and alcohol and/or drug abuse records. Protected health information may be written, oral, or electronic. This form does not permit the use or disclosure of psychotherapy notes or the disclosure of information concerning whether I, my spouse or my dependent child(ren) have obtained a test for the presence of HIV antigen or nonantigenic products of HIV or an antibody to HIV or what the results of this test were.
II. Purpose of this Authorization Form
By signing this form, I, my spouse and my dependent child(ren) authorize the use and disclosure of protected health information for the purposes of pre-enrollment underwriting or risk-rating of health insurance coverage for me, my spouse and my dependent child(ren), to determine eligibility for enrollment or benefits under a health plan or to allow the insurer to conduct utilization review and quality improvement activities (“Purpose”).
III. Entities Authorized to Use and Disclose My Protected Health Information
Insurers: I hereby authorize the following insurers, their reinsurers, and their legal representatives (“Insurers”) to receive, use, and disclose my, my spouse’s and my dependent child(ren)’s protected health information for the Purpose listed above:
Insurer: __________________________________________ |
Insurer: __________________________________________ |
Insurer: __________________________________________ |
Insurer: __________________________________________ |
I authorize the Insurers to disclose my, my spouse’s and my dependent child(ren)’s protected health information: between themselves, to reinsuring companies, and to the plan administrator (if other than the employer), plan sponsor (if other than the employer), insurance intermediaries, or other persons or organizations performing business or legal services in connection with the Purpose above.
I further authorize any licensed physician, medical practitioner, health care provider, hospital, clinic, or other medical or medically related facility, insurance or reinsuring company, Medical Information Bureau, Inc., consumer reporting agency, or other organization, institution, or person that has any record or knowledge of me, my spouse or my dependent(s), to give to Insurers any and all protected health information about me, my spouse, or my dependent(s) to be covered concerning diagnosis, treatment and prognosis for any physical or mental condition, history or character, general reputation, personal trait, and mode of living, including, but not limited to, all medical and health care records, but not including whether I, my spouse or my dependent(s) obtained a test for the presence of HIV antigen or nonantigenic products of HIV or what the results of this test were.
I, my spouse and my dependent child(ren) understand that protected health information described in this form may be used by, or disclosed to or by, organizations and persons who are not subject to federal or state privacy laws.
IV. Term of Authorization
I agree this Authorization shall be valid for two and one half (2 ½) years from the latest signature date below.
V. Right to Revoke
I understand I, my spouse or my dependent child(ren) may revoke this authorization at any time by giving advance written notice to Insurers. Revocation of this authorization form will not affect actions Insurers and others took in reliance on this form prior to the written notice of revocation.
I HAVE HAD FULL OPPORTUNITY TO READ AND CONSIDER THIS FORM. I UNDERSTAND THAT, BY SIGNING THIS FORM, I AUTHORIZE THE USES AND DISCLOSURES OF PROTECTED HEALTH INFORMATION DESCRIBED IN THIS FORM. I UNDERSTAND THAT I MAY ONLY REVOKE AUTHORIZATION FOR MYSELF OR MY MINOR CHILD(REN) UNLESS MY MINOR CHILD(REN) HAS RECEIVED TREATMENT WITHOUT MY CONSENT, CONSISTENT WITH STATE LAW. (CONTINUED ON THE NEXT PAGE.)
_______________________________________ |
_____________________ |
_________________________________ |
Signature of Adult Applicant |
Date signed |
Printed Name |
_______________________________________ |
_____________________ |
_________________________________ |
Signature of Spouse (if applicable) |
Date signed |
Printed Name |
Uniform Employee Application |
Page 8 of 9 |
|