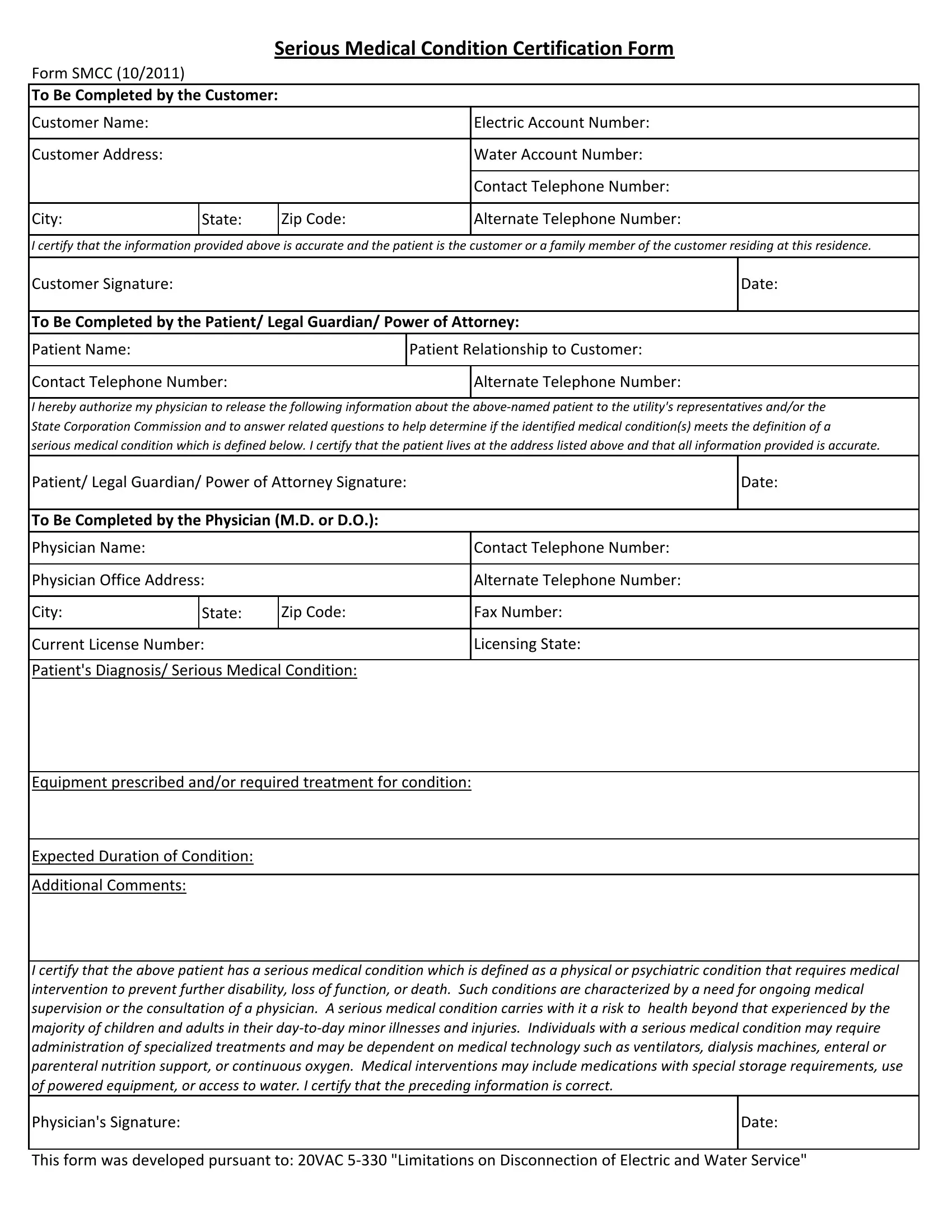
In today's complex healthcare and utility landscape, the intersection of medical needs and utility services has grown increasingly important, particularly for individuals facing serious medical conditions. The Serious Medical Condition Certification Form (SMCC), updated in October 2011, serves as a critical document in this intersection, designed to protect patients by preventing the disconnection of their electric and water services. This form requires detailed information from three key parties: the customer, the patient (or their legal guardian/power of attorney), and the physician—each playing a pivotal role in certifying the patient's medical needs. For customers, this includes verifying their relationship to the patient and providing essential account and contact information. Patients or their representatives are tasked with authorizing physicians to disclose medical information relevant to the patient's condition. The most crucial segment of the form is completed by a physician (M.D. or D.O.), who must outline the patient's diagnosis, any prescribed equipment or treatments, and the expected duration of the condition, hence confirming the presence of a serious medical condition as defined by the document. This definition encompasses a range of conditions that significantly surpass the health risks of minor illnesses by necessitating medical intervention to prevent disability, loss of function, or death. The form acts as a safeguard, ensuring that those dependent on life-sustaining medical equipment or treatments maintain uninterrupted access to electricity and water, thereby acknowledging the profound impact of utility services on the health and well-being of individuals with serious medical conditions.
| Question | Answer |
|---|---|
| Form Name | Form Smcc |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | med_cert scc serious medical condition certification form |
|
|
Serious Medical Condition Certification Form |
||
Form SMCC (10/2011) |
|
|
|
|
|
|
|||
To Be Completed by the Customer: |
|
|||
|
|
|
|
|
Customer Name: |
|
|
|
Electric Account Number: |
|
|
|
|
|
Customer Address: |
|
|
|
Water Account Number: |
|
|
|
|
|
|
|
|
|
Contact Telephone Number: |
|
|
|
|
|
City: |
State: |
|
Zip Code: |
Alternate Telephone Number: |
|
|
|
|
|
I certify that the information provided above is accurate and the patient is the customer or a family member of the customer residing at this residence.
Customer Signature: |
|
|
Date: |
|
|
|
|
To Be Completed by the Patient/ Legal Guardian/ Power of Attorney: |
|||
|
|
||
Patient Name: |
Patient Relationship to Customer: |
||
|
|
|
|
Contact Telephone Number: |
|
Alternate Telephone Number: |
|
|
|
|
|
I hereby authorize my physician to release the following information about the
Patient/ Legal Guardian/ Power of Attorney Signature: |
|
Date: |
||
|
|
|
|
|
To Be Completed by the Physician (M.D. or D.O.): |
|
|
||
|
|
|
|
|
Physician Name: |
|
|
Contact Telephone Number: |
|
|
|
|
||
Physician Office Address: |
|
Alternate Telephone Number: |
||
|
|
|
|
|
City: |
State: |
Zip Code: |
Fax Number: |
|
|
|
|
|
|
Current License Number: |
|
Licensing State: |
||
|
|
|
|
|
Patient's Diagnosis/ Serious Medical Condition: |
|
|
||
Equipment prescribed and/or required treatment for condition:
Expected Duration of Condition:
Additional Comments:
I certify that the above patient has a serious medical condition which is defined as a physical or psychiatric condition that requires medical intervention to prevent further disability, loss of function, or death. Such conditions are characterized by a need for ongoing medical supervision or the consultation of a physician. A serious medical condition carries with it a risk to health beyond that experienced by the majority of children and adults in their
Physician's Signature: |
Date: |
|
|
This form was developed pursuant to: 20VAC