Our PDF editor helps make writing forms simple. It is very effortless to enhance the Gid 103 Al Form file. Adhere to all of these steps if you need to achieve this:
Step 1: First, click the orange "Get form now" button.
Step 2: As soon as you have accessed the Gid 103 Al Form edit page, you'll discover all options you may take with regards to your document in the top menu.
Type in the necessary material in each part to fill out the PDF Gid 103 Al Form
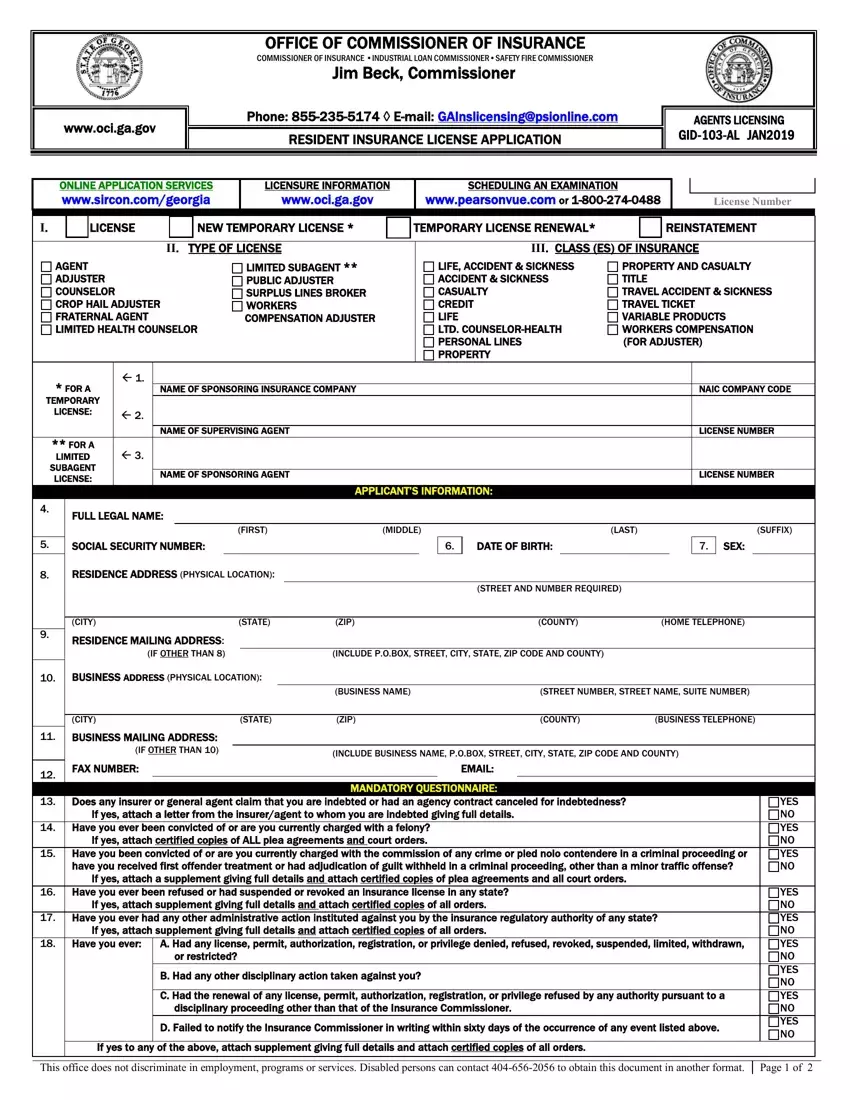
Complete the RESIDENCE, ADDRESS, PHYSICAL, LOCATION STREET, AND, NUMBER, REQUIRED CITY, STATE, ZIP, COUNTY, HOME, TELEPHONE RESIDENCE, MAILING, ADDRESS, IF, OTHER, THAN BUSINESS, ADDRESS, PHYSICAL, LOCATION CITY, BUSINESS, MAILING, ADDRESS, IF, OTHER, THAN FAX, NUMBER BUSINESS, NAME STREET, NUMBER, STREET, NAME, SUITE, NUMBER and ZIP section with all the information asked by the system.
Describe the key information in the YES, NOYES, NOYES, NOYES, NOYES, NOYES, NO and Page, of field.

The APPLICANTS, ATTESTATION YES, NOYES, NOYES, NOYES, NOYES, NO SIGNATURE, OF, APPLICANT DATE, NOTARY, SEAL, SIGNATURE, REQUIRED Seal, and SPONSORS, CERTIFICATE area is the place where all parties can indicate their rights and responsibilities.
Prepare the template by reviewing all of these sections: Name, Title, Signature, INSTRUCTIONS, BOND, CITIZENSHIP, AFFIDAVIT FINGERPRINTS, VARIABLE, PRODUCTS COUNSELOR, LICENSE FOR, ONE, CLASS, MAJOR, LINE, OF, INSURANCE AGENT, LICENSE TEMPORARY, LICENSE LIMITEDSUBAGENT, LICENSE and FEE, SCHEDULE
Step 3: Click the "Done" button. Now you can export your PDF file to your electronic device. Additionally, you may forward it through electronic mail.
Step 4: In order to avoid potential forthcoming concerns, ensure that you hold no less than a couple of copies of each separate form.
