The HMSA Quest Prior Authorization form serves as a critical tool in the process of obtaining coverage for specific medications under the HMSA Quest (Medicaid) program, with explicit focus on the medication Campral (acamprosate calcium). Created to ensure that medications are used in a safe, effective, and appropriate manner, this document requires detailed information about the patient’s condition, as well as the medication requested. Dated August 6, 2013, the form adheres to strict HIPAA regulations to maintain patient confidentiality, mandating that it be completed, signed, and then faxed to CVS/Caremark for processing. It embodies a series of criteria that need to be met before authorization for coverage can be granted, including clinical diagnosis, previous treatment attempts, and the planned duration of therapy. Questions designed to assess the appropriateness of Campral based on prior alcohol dependence treatment, potential renal impairment, and the inclusion in a broader psychosocial treatment program highlight the form’s comprehensive approach to evaluating treatment necessity and efficacy. With specific instructions for direct communication with CVS/Caremark for questions regarding the process, it exemplifies a streamlined mechanism aimed at ensuring that patients receive the most suitable medication support within the framework of Medicaid provisions.
| Question | Answer |
|---|---|
| Form Name | HMSA Quest Prior Authorization Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 72 |
| Avg. time to fill out | 14 min 43 sec |
| Other names | hmsa quest prior authorization medication, mavenclad prior authorization criteria, hmsaq quest pa drug, empire blue cross blue shield pdf prior auth request forms |
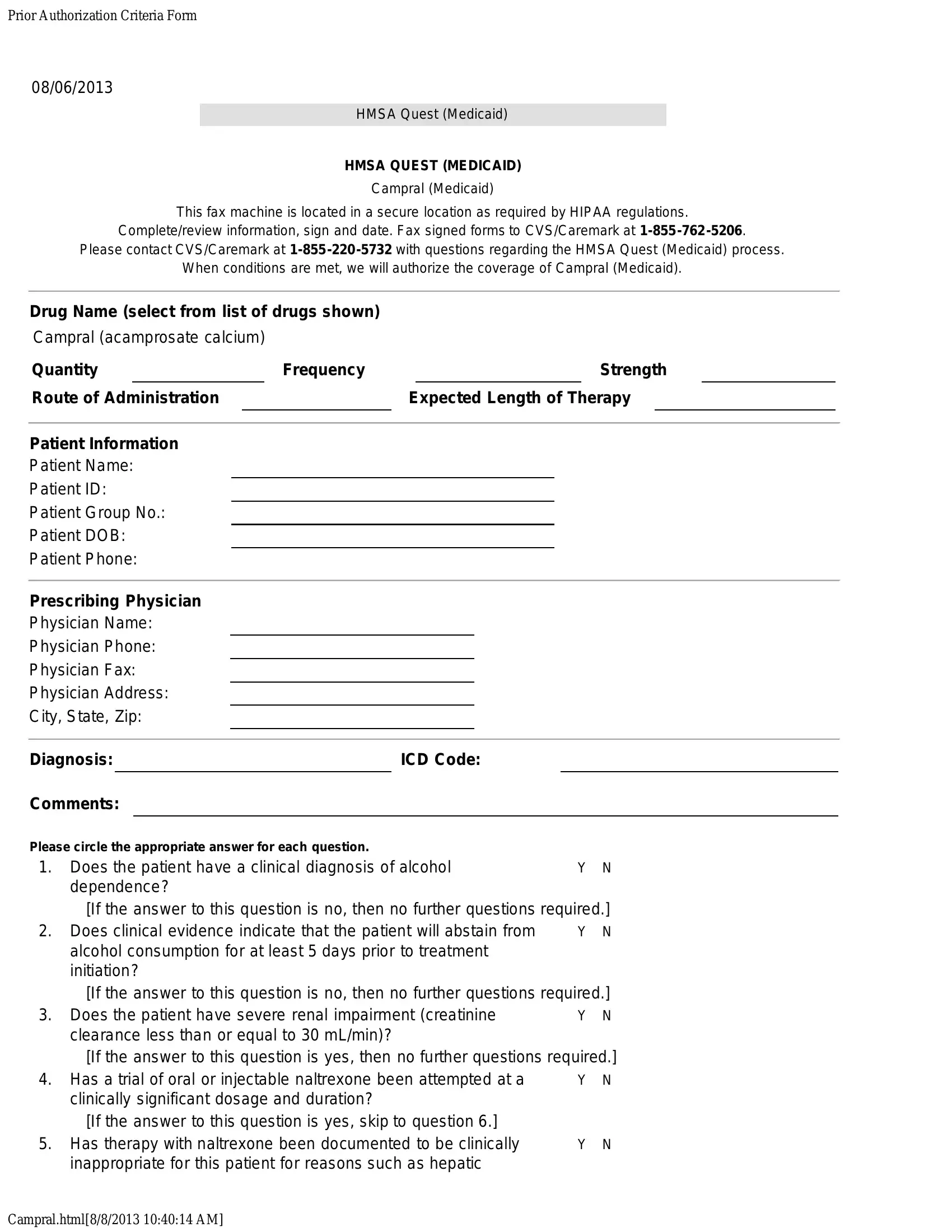
Prior Authorization Criteria Form
08/06/2013
HMSA Quest (Medicaid)
HMSA QUEST (MEDICAID)
Campral (Medicaid)
This fax machine is located in a secure location as required by HIPAA regulations.
Complete/review information, sign and date. Fax signed forms to CVS/Caremark at
Please contact CVS/Caremark at
When conditions are met, we will authorize the coverage of Campral (Medicaid).
Drug Name (select from list of drugs shown)
Campral (acamprosate calcium)
Quantity |
|
Frequency |
|
|
|
|
|
Strength |
|
|
||||
Route of Administration |
|
Expected Length of Therapy |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Information |
|
|
|
|
|
|
|
|
|
|
||||
Patient Name: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient ID: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Group No.: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient DOB: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Phone: |
|
|
|
|
|
|
|
|
|
|
||||
Prescribing Physician |
|
|
|
|
|
|
|
|
|
|
||||
Physician Name: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Phone: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Fax: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Address: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City, State, Zip: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|||||
Diagnosis: |
|
ICD Code: |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Comments: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please circle the appropriate answer for each question.
1. |
Does the patient have a clinical diagnosis of alcohol |
Y |
N |
|
dependence? |
|
|
|
[If the answer to this question is no, then no further questions required.] |
||
2. |
Does clinical evidence indicate that the patient will abstain from |
Y |
N |
|
alcohol consumption for at least 5 days prior to treatment |
|
|
|
initiation? |
|
|
|
[If the answer to this question is no, then no further questions required.] |
||
3. |
Does the patient have severe renal impairment (creatinine |
Y |
N |
|
clearance less than or equal to 30 mL/min)? |
|
|
|
[If the answer to this question is yes, then no further questions required.] |
||
4. |
Has a trial of oral or injectable naltrexone been attempted at a |
Y |
N |
|
clinically significant dosage and duration? |
|
|
|
[If the answer to this question is yes, skip to question 6.] |
|
|
5. |
Has therapy with naltrexone been documented to be clinically |
Y |
N |
|
inappropriate for this patient for reasons such as hepatic |
|
|
Campral.html[8/8/2013 10:40:14 AM]

Prior Authorization Criteria Form |
|
insufficiency or chronic pain medication use? |
|
6. Will Campral administration be a part of a comprehensive |
Y N |
psychosocial treatment program for this patient? |
|
I affirm that the information given on this form is true and accurate as of this date.
Prescriber (Or Authorized) Signature and Date
Campral.html[8/8/2013 10:40:14 AM]