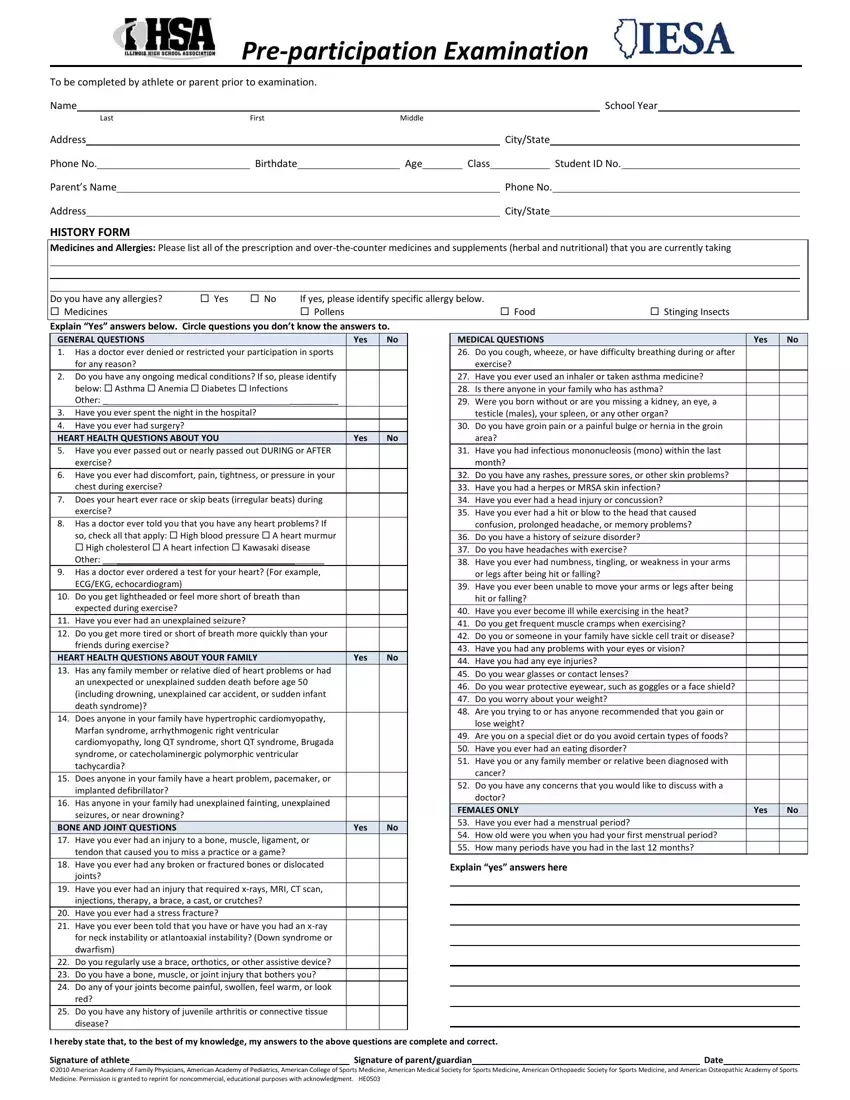
Understanding the Illinois Pre Participation Physical form is crucial for athletes, parents, and guardians aiming for participation in sports activities. This comprehensive form, diligently designed to ensure the health and safety of student-athletes, encapsulates vital information covering medical history, general questions about the athlete's health, a scrutinizing examination of heart health, and inquiries into any past bone and joint injuries. Notably, it goes beyond the surface, looking into potential allergies, ongoing medications – both prescription and over-the-counter, and any historical familial health issues that might influence the athlete's ability to perform. The form doesn't stop there; it delves into specifics concerning respiratory conditions, visual health, nutrition, and even mental health aspects related to sports performance. Completed with sections dedicated to both the physical examination, including musculoskeletal, neurological, and cardio evaluations, and a segment on steroid testing policy consent, it's a testament to the multiplex considerations taken to safeguard the well-being of participants in interscholastic sports. By signing this document, athletes and their guardians not only affirm the accuracy of the information provided but also agree to comply with the policies set by the Illinois High School Association, marking an essential step towards a secure and health-conscious sporting environment.
| Question | Answer |
|---|---|
| Form Name | Illinois Pre Participation Physical Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 216 |
| Avg. time to fill out | 21 min 53 sec |
| Other names | ihsa sports 2021, ihsa sports form, printable sports physical form illinois, illinois sports physical form 2020 |
