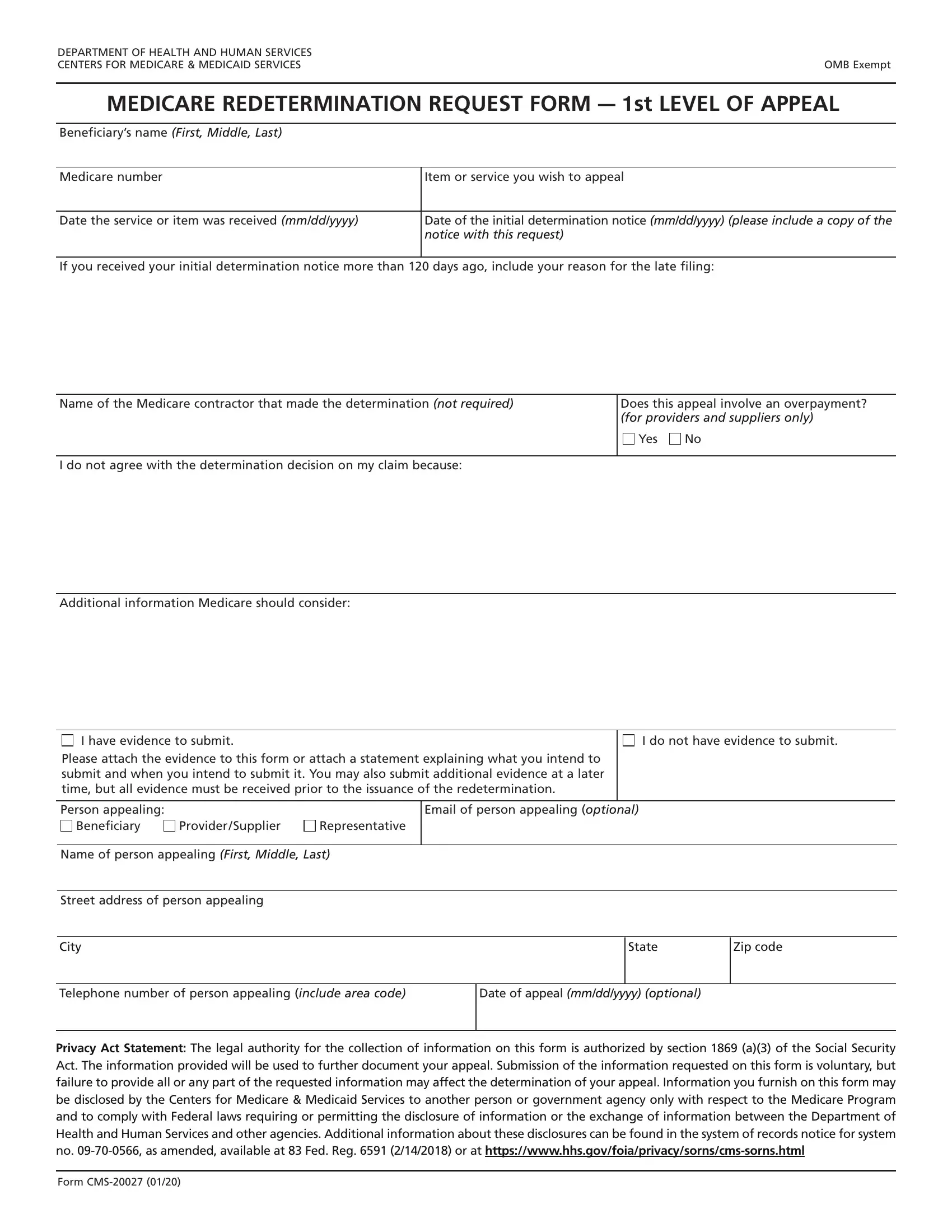
Navigating through the Medicare system can be challenging, especially when disputes arise regarding coverage decisions. The Medicare Redetermination Request Form, also known as Form CMS-20027, serves as a critical tool for individuals seeking to challenge these decisions. Managed by the Department of Health and Human Services and overseen by the Centers for Medicare & Medicaid Services, this form marks the first level of appeal in the Medicare appeals process. It is designed for beneficiaries, providers, or suppliers who disagree with an initial determination regarding Medicare coverage or payment. The form requires detailed information, including the beneficiary's name, Medicare number, the service or item being appealed, and the date the service was received. An essential part of this process involves submitting evidence to support the appeal, which can drastically influence the outcome. Additionally, it outlines the necessity of including the date of the initial determination notice and underscores the importance of filing the appeal within 120 days of receiving this notice to avoid the need for an explanation for any delay. This form not only facilitates a structured appeal process but also upholds the individual's right to challenge decisions made by Medicare contractors. The provided Privacy Act Statement reassures applicants about the confidentiality and intended use of their information, emphasizing that submission is voluntary but crucial for the appeal's consideration. As such, the Medicare Redetermination Request Form plays a pivotal role in ensuring that disputes regarding Medicare decisions are addressed promptly and effectively.
| Question | Answer |
|---|---|
| Form Name | Medicare Request Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | how to form cms 20027, cms 20027 form, medicare form cms 20027, forms for medicare |