
Dealing with PDF files online is actually very simple with our PDF editor. You can fill out death certificate download here in a matter of minutes. Our tool is constantly developing to grant the best user experience attainable, and that's due to our resolve for continuous improvement and listening closely to comments from users. All it takes is several basic steps:
Step 1: Open the PDF file in our tool by hitting the "Get Form Button" at the top of this webpage.
Step 2: With our online PDF file editor, it is easy to do more than merely fill out forms. Edit away and make your documents appear high-quality with custom text incorporated, or tweak the original content to excellence - all backed up by the capability to insert almost any pictures and sign the document off.
If you want to fill out this PDF document, ensure that you provide the information you need in every area:
1. It is crucial to complete the death certificate download accurately, thus pay close attention while filling out the sections comprising these particular blank fields:
2. Just after performing the previous section, head on to the subsequent step and fill in the essential details in all these fields - a INFORMANTS NAME TypePrint, b RELATIONSHIP TO DECEDENT, c MAILING ADDRESS Street and, METHOD OF DISPOSITION Burial, Donation Removal Storage Specify, a PLACE OF DISPOSITION Name of, b LOCATION City or Village State, SIGNATURE OF MORTUARY SCIENCE, LICENSE NUMBER of Licensee, NAME AND ADDRESS OF FUNERAL, a CERTIFIER Check only one, Certifying Physician To the best, manner stated, Medical Examiner On the basis of, and occurred at the time date and.
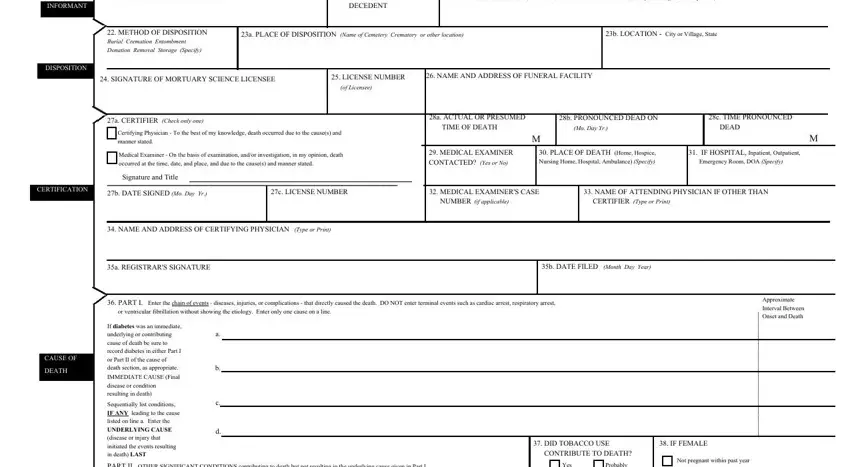
Be really attentive when filling in b RELATIONSHIP TO DECEDENT and Certifying Physician To the best, since this is the part where most users make a few mistakes.
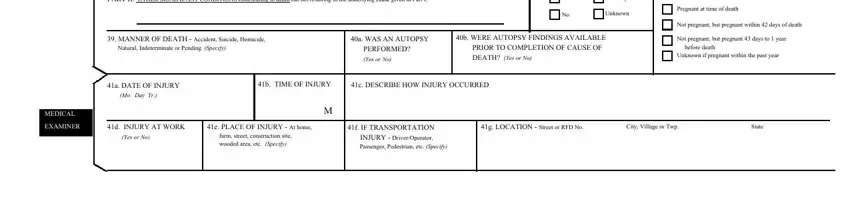
3. Completing PART II OTHER SIGNIFICANT, Yes, Probably, Unknown, Pregnant at time of death, MANNER OF DEATH Accident Suicide, a WAS AN AUTOPSY PERFORMED Yes or, b WERE AUTOPSY FINDINGS AVAILABLE, Not pregnant but pregnant within, Not pregnant but pregnant days to, before death, Unknown if pregnant within the, a DATE OF INJURY Mo Day Yr, b TIME OF INJURY, and c DESCRIBE HOW INJURY OCCURRED is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Step 3: Right after taking another look at the entries, hit "Done" and you're good to go! Right after getting afree trial account at FormsPal, you will be able to download death certificate download or send it through email directly. The PDF will also be readily accessible through your personal account with your modifications. FormsPal provides secure form completion with no personal data record-keeping or distributing. Feel at ease knowing that your data is in good hands here!