
of178 can be filled out online without any problem. Simply open FormsPal PDF editor to get it done quickly. The tool is continually maintained by our staff, receiving awesome functions and becoming greater. All it takes is just a few simple steps:
Step 1: Firstly, open the tool by pressing the "Get Form Button" above on this webpage.
Step 2: Using our advanced PDF file editor, you are able to do more than just complete blank form fields. Express yourself and make your documents seem high-quality with custom text put in, or optimize the original input to excellence - all supported by an ability to insert your own photos and sign the file off.
It's straightforward to finish the form using out practical guide! Here's what you want to do:
1. While completing the of178, make certain to include all important blanks within the corresponding form section. It will help to facilitate the process, which allows your information to be handled fast and properly.
2. Now that this segment is done, it's time to insert the necessary specifics in Applicant or Employee Consent and, I certify that all of the, Signature Do not print, Date month day year, Part B TO BE COMPLETED BEFORE, Purpose of examination, Position Title Series and Grade, Preplacement, Other Specify, Brief description of what the, US Office of Personnel Management, and Optional Form April Formerly SF in order to progress to the third step.
3. Completing US Office of Personnel Management, Page of, Optional Form April Formerly SF, Name, Last digits of Social Security, and Date is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

4. The fourth paragraph arrives with the next few blank fields to fill out: a Functional Requirements, Heavy lifting pounds and over, Repeated bending hours, Moderate lifting pounds, Climbing legs only hours, Both eyes required, Depth perception, Light lifting under pounds, Climbing use of legs and arms, Ability to distinguish basic colors, Heavy carrying pounds and over, Both legs required, Operation of crane truck tractor, Ability for rapid mental and, and Ability to use and desirability of.
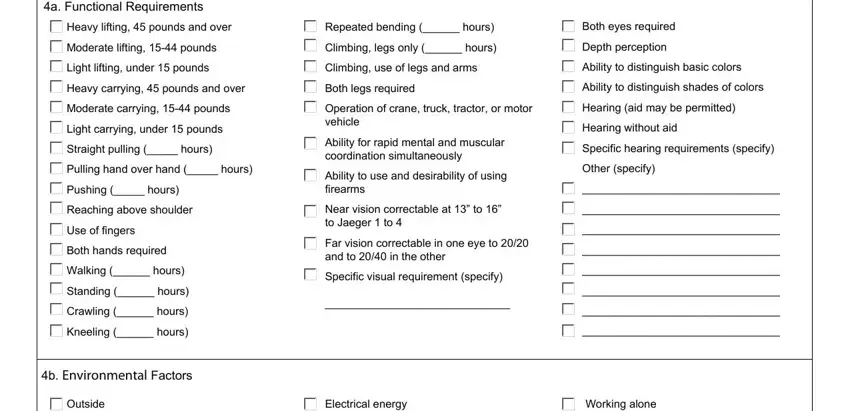
Be very attentive while filling in Heavy lifting pounds and over and Depth perception, since this is where a lot of people make mistakes.
5. This document has to be completed by filling out this part. Here you will see a detailed set of blanks that require accurate information for your form usage to be accomplished: Outside and inside, Excessive heat, Excessive cold, Excessive humidity, Slippery or uneven walking surfaces, Protracted or irregular hours of, Working around machinery with, Other specify, Working around moving objects or, Working on ladders or scaffolding, Excessive dampness or chilling, Working below ground, Dry atmospheric conditions, Unusual fatigue factors specify, and Excessive noise intermittent.
Step 3: Right after proofreading your fields, click "Done" and you are all set! After starting a7-day free trial account here, you'll be able to download of178 or email it without delay. The form will also be at your disposal from your personal cabinet with your every change. FormsPal provides safe form tools devoid of data record-keeping or any sort of sharing. Be assured that your details are in good hands with us!